

I have a Wahoo KICKR Core 2 in the corner of my home gym. Most weeks it sees me twice. Once for Zone 2, sometimes for the Norwegian 4×4 protocol I wrote about back in the fall. I picked cycling because my knees and one toe joint will not let me run, not because I had read anything specific about what cycling does to the brain.
Then a new dataset landed that made me look at the bike differently. A study of 479,723 adults in the UK Biobank, published last June in JAMA Network Open, asked a question most exercise research dodges: not “is exercise good for your brain,” but “does the type of exercise matter for dementia risk?” The answer they got, in plain numbers, was that cyclists had a 22% lower risk of Alzheimer’s disease and a 40% lower risk of young-onset dementia compared to people who got around by car or bus.
That’s the headline you may have seen in the Telegraph this weekend, which got the journal wrong (it’s JAMA Network Open, not JAMA proper) and overstated who led the study. The underlying numbers are real. They’re also more complicated than the headline.
What the study actually measured
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
The paper is called Active Travel Mode and Incident Dementia and Brain Structure, Hou and colleagues, Tongji Medical College in Wuhan, with a co-author at the University of Sydney’s School of Public Health. They followed nearly half a million UK Biobank participants for a median of 13.1 years and grouped them by how they mostly got around: nonactive (car, bus), walking, mixed walking, and cycling or mixed cycling.
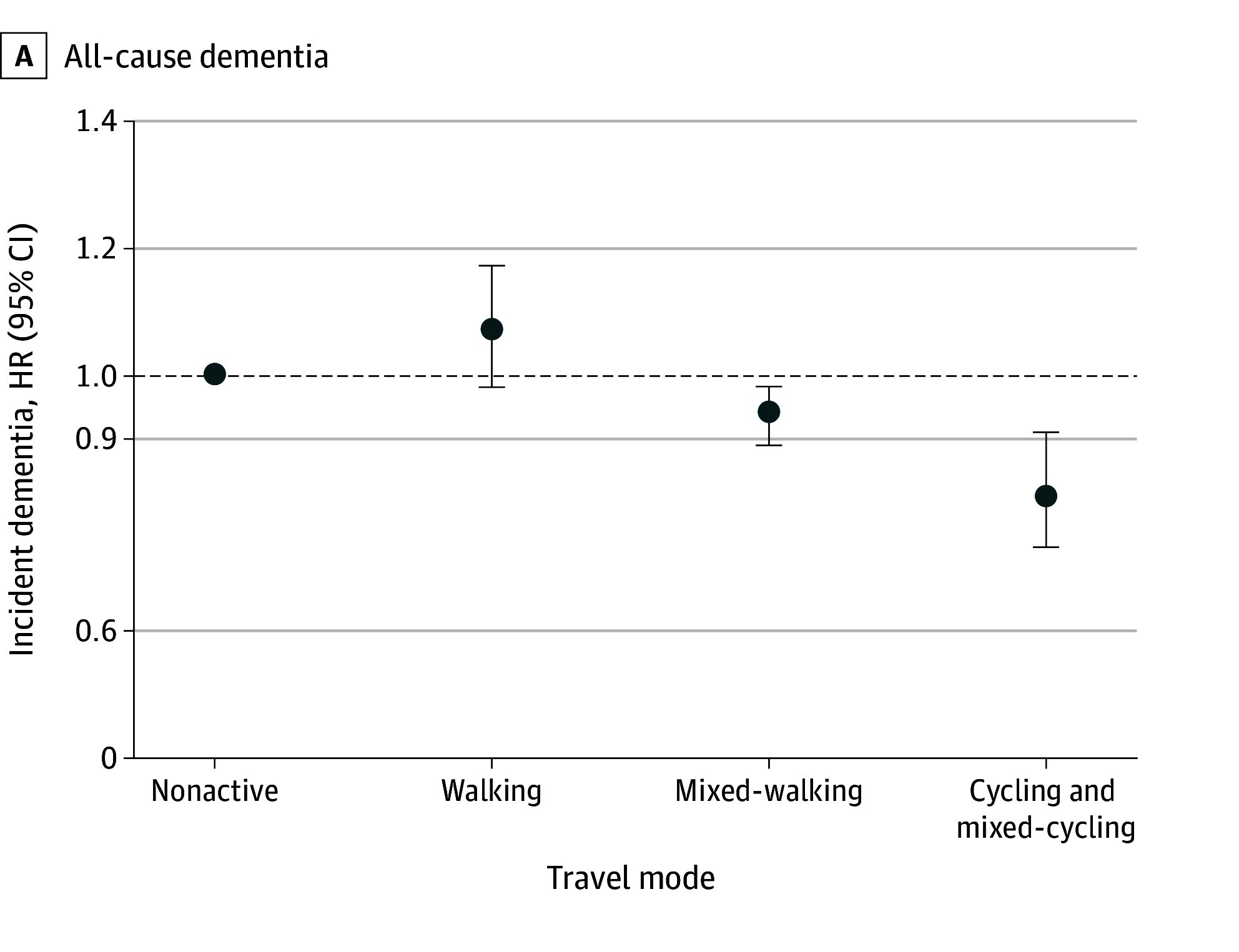
Compared to nonactive travel, the cycling and mixed-cycling group had:
A 19% lower risk of all-cause dementia (HR 0.81, 95% CI 0.73 to 0.91).
A 22% lower risk of Alzheimer’s disease (HR 0.78, 95% CI 0.66 to 0.92).
A 40% lower risk of young-onset dementia, the kind diagnosed before age 65 (HR 0.60, 95% CI 0.38 to 0.95).
A 17% lower risk of late-onset dementia (HR 0.83, 95% CI 0.75 to 0.93).
A measurably larger hippocampus on MRI (β 0.05, 95% CI 0.02 to 0.08).
The situation is cleaner as a forest plot than as a list of numbers. Each dot is the hazard ratio for that travel mode compared to the nonactive reference. The vertical bars are the 95% confidence intervals. Walking lands at or slightly above no-activity. Mixed-walking sits just below. Cycling is the only mode where the entire confidence interval lives under the reference line.
The hippocampus is the seahorse-shaped structure deep in your brain where short-term memory gets converted to long-term memory. It is also where Alzheimer’s first becomes visible on imaging. A larger one is generally a healthier one for people our age.
Walking helped less than cycling. The benefit for walking alone, in this dataset, was smaller and less consistent.
The APOE caveat nobody is talking about
This is the part the news writeups conveniently glossed over, and that you should know about, because for a slice of you reading this it matters a lot.
The protective effect of cycling depended on your APOE genotype. APOE ε4 is the well-known genetic risk variant for Alzheimer’s. Roughly 15 to 25% of people carry at least one copy. The researchers tested whether the cycling benefit held up in ε4 carriers, and the answer was: not as clearly.
For people without APOE ε4, the all-cause dementia hazard ratio in cyclists was 0.74 (95% CI 0.63 to 0.87). That is a statistically significant 26% reduction in risk.
For people with APOE ε4, the hazard ratio was 0.88 (95% CI 0.76 to 1.02). The confidence interval crosses 1.0. That means the result is not statistically significant. Cycling may still help ε4 carriers, but the effect is smaller and the data is not strong enough to say so confidently.
Two honest takeaways from this. First, if you have ever done a consumer genetics test that reported APOE (which, fair, most people haven’t), your status is worth knowing for context. Second, an ε4 result is not a reason to stop cycling. The cardiovascular benefits are real and large for everyone. It is a reason to be realistic about how much of your dementia risk you can move with any single intervention.
Why cycling might work better than walking
The paper itself doesn’t fully explain why cycling outperforms walking. The likely answer is that cycling is doing two things at once.
The first is cardiovascular. You are working continuously, using the largest muscles in your body, for sustained periods. That trains your aerobic capacity in a way few daily activities do. Aerobic fitness measured as VO2max is one of the most reliable predictors of all-cause mortality we have, and it correlates with brain volume and cognitive function in older adults independent of other factors. The Norwegian 4×4 protocol I wrote about is one of the cleanest ways to actually move that number. You don’t need to run to do it.
The second is what researchers call dual-tasking. Cycling on a road requires you to track traffic, anticipate hazards, plan your route, and modulate your effort. You can’t passively follow a satnav while cycling the way you can while walking. That sustained cognitive load while exercising appears to be a separate brain-health input, independent of the cardiovascular effect. Indoor cycling on a trainer loses some of that, which is an honest tradeoff worth naming. The mechanism is probably partially offset by the safer recovery context and the easier consistency.
There is also a likely BDNF story underneath all of this. BDNF (brain-derived neurotrophic factor) is a molecule the brain releases in response to aerobic exercise that helps existing brain cells survive and supports the formation of new connections between them. A small University College London randomized trial published this March is worth being precise about: a 12-week cycling intervention did not raise resting BDNF levels, but it did significantly enhance the acute BDNF spike that follows a single exercise bout. The training effect, in other words, isn’t that you walk around with more BDNF in your blood. It’s that every time you actually exercise, your trained brain produces a bigger BDNF response than your untrained brain would have. That acute response correlated with VO2max gains and with measurable changes in prefrontal cortex activity during attention tasks. BDNF isn’t a magic pathway, but it is one of the cleaner mechanistic candidates for how exercise protects the aging brain.
The counter-evidence I have to mention
If I only handed you the JAMA Network Open paper, I would be doing the same thing the Telegraph did, which is treat one good observational result as if it settled the question.
It hasn’t.
Earlier this month, JAMA Neurology published a randomized controlled trial by Zhang, Vidoni and colleagues in 513 older adults with hypertension plus either a family history of dementia or self-reported cognitive concerns. Over 24 months, participants were randomized in a 2×2 factorial design to aerobic exercise training, intensive vascular risk reduction (systolic blood pressure pushed below 130 mm Hg and LDL lowered with atorvastatin), both, or usual care. The expectation was that the active interventions would slow cognitive decline. The actual result was that they did not. None of the intervention arms outperformed usual care on the primary cognitive outcome.
This is a real result, not a footnote. And it sits in some tension with the cycling paper.
How to hold both at once: the cycling paper is observational, which means it can identify associations but not prove causation. People who cycle regularly in middle age are systematically different from people who don’t, in ways that don’t all wash out with statistical adjustment. The RCT is causally cleaner but tested a specific late-life intervention package, not lifelong cycling, and the exercise dose may not have been strong enough to produce a real fitness signal. Both findings can be true. Cycling as a long-term habit over decades may genuinely lower dementia risk through cardiovascular, neurotrophic, and dual-task mechanisms. Adding a structured exercise-and-medication program to a 68-year-old already showing cognitive vulnerability may not be enough to reverse what was set up over the preceding fifty years.
That second sentence is the harder pill. Most of what cycling can do for your brain probably has to happen before the symptoms show up, not after.
What I’m actually going to do about it
Three things, in order.
First, I am going to keep cycling, mostly on the KICKR. My wife and I have talked about outdoor riding more than once, and we have both landed in the same place: cars in our area do not give cyclists enough room, and the risk-adjusted math doesn’t work for us right now. So the indoor sessions get the bulk of the load. The cardiovascular benefit is fully available indoors. The dual-tasking benefit is harder to replicate on a trainer, but a structured Zwift session in a group ride or a route that demands attention to power targets and gradient changes captures more of it than zoning out to a podcast. Honest: indoor cycling is probably giving up some of the brain-specific benefit the study saw. It is also keeping me alive long enough to use the brain in the first place.
Second, I am going to keep treating cardiovascular fitness as the single most important thing I do for long-term health (I am aware this is the kind of line every 50-year-old delivers right before injuring themselves). Not because cycling specifically is magical, but because aerobic capacity is one of the few biomarkers that responds quickly to training and tracks downstream outcomes cleanly. I feel pretty good about my lipid panel. The DIY longevity protocol post has the rest of what I do if you want the full menu.
Third, if you don’t already know your APOE status, it is worth thinking about. Not because it changes whether you should cycle, but because it changes how aggressive you might want to be about every other lever you have, from sleep to blood pressure to LDL to social connection. If you are ε4 positive, the cycling alone math may not pull as hard for you, and the case for layering interventions gets stronger.
What to do this week
If you don’t currently cycle, start with whatever bike you can get on. Outdoor riding has the strongest dual-tasking case if your local roads are safe enough that you’d be comfortable having your spouse watch you head out. If they aren’t, an indoor trainer or a Concept2 rower captures the cardiovascular benefit, and a route-tracking app like Zwift captures more of the dual-tasking benefit than a passive screen would. None of those options beat not cycling at all.
Aim for the kind of consistency this study tracked, which was “most often” using cycling as a mode of transport over the past four weeks. Translated into a home gym: two or three sessions a week, 30 to 45 minutes each, varying intensity. The Norwegian 4×4 protocol is one way to add a high-intensity dose without ruining your knees.
If you are 50 and you have been letting your bike collect dust because you stopped commuting on it, this is the nudge to put it back into rotation, indoors or out. The cardiovascular benefits start within weeks. The brain benefits, if the cycling paper is right, accumulate over years and decades, which means now is exactly when they start counting.
If you are ε4 positive and feeling discouraged, the right reading of this paper is not “cycling won’t help me.” It is “cycling alone won’t be enough to overcome my genetic risk, so I should layer it with everything else.” That is a more demanding read but a more useful one.
I’ll be on the KICKR tomorrow morning either way. The math on doing nothing is worse than the math on imperfect evidence.
Primary sources
- Hou C, Zhang Y, Zhao F, Lv Y, Luo M, Pan C, Ding D, Chen L. Active Travel Mode and Incident Dementia and Brain Structure. JAMA Netw Open. 2025 Jun 2;8(6):e2514316. PubMed · DOI: 10.1001/jamanetworkopen.2025.14316
- Zhang R, Vidoni E, Vongpatanasin W, et al. Effects of Exercise and Intensive Vascular Risk Reduction on Cognitive Function in Older Adults: A Randomized Clinical Trial. JAMA Neurol. 2026 May 1;83(5):424-434. PubMed · DOI: 10.1001/jamaneurol.2026.0359
- Ronca F, Xu C, Kong E, et al. BDNF relates to prefrontal cortex activity in the context of physical exercise. Brain Res. 2026 Jun 15;1881:150253. PubMed · DOI: 10.1016/j.brainres.2026.150253
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.