

I have been on Zepbound for eighteen months. Today the drug that may replace it just showed its hand.
Get the free Bloodwork Decoder
I made the one-page cheat sheet I wish I’d had at my first physical: what every number on your labs actually means, what’s worth aiming for at 50, and what to ask your doctor. Subscribe free and I’ll send it straight to your inbox. No spam, nothing to sell.
When I started Zepbound in late 2024 I knew tirzepatide was not the end of the road. The pharmacology was already pointing somewhere further. Tirzepatide had taken the original GLP-1 agonist class (semaglutide and the others) and added a second receptor (GIP), which produced an extra ten percentage points of weight loss in head-to-head trials. The obvious next step was to add a third receptor (glucagon), and Eli Lilly had a molecule that did exactly that already in Phase 2 clinical trials. It was called LY3437943, since renamed retatrutide.
Today Lilly reported the topline results of TRIUMPH-1, the pivotal Phase 3 obesity trial for retatrutide. The numbers are real. Patients on the highest dose lost 28.3 percent of their body weight over 80 weeks. In the subgroup with severe obesity (BMI ≥35) followed for two years, the loss was 30.3 percent. To anchor that number: people who have gastric bypass surgery lose about 30 to 35 percent of their body weight at two years. This is the first non-surgical intervention to produce surgery-equivalent weight loss in severely obese patients in a randomized trial.
LLY stock is up about 2 percent today, adding roughly twenty billion dollars in market value. The New York Times ran the story under the headline “Experimental Drug Yields Dramatic Weight Loss.” The major outlets are aligned on the framing: retatrutide is the most powerful obesity drug yet tested.
I am going to walk through what the trial actually showed, why three receptors might beat two, the timeline for when you can legally get this drug in the United States, and the uncomfortable fact that thousands of bodybuilders and biohackers have already been on it for over a year through gray-market peptide retailers. The last part is the story most coverage will dance around. I am going to be direct about it because that conversation is happening in r/retatrutide and on every men’s-health forum and your readers (and my Zepbound-using neighbors) deserve honest framing about what they will see online over the next week.
What the numbers actually say
TRIUMPH-1 is the obesity registrational Phase 3 trial in Lilly’s broader TRIUMPH program. The full program has four Phase 3 trials covering obesity, type 2 diabetes, established cardiovascular disease, and knee osteoarthritis, with a separate dedicated cardiovascular outcomes trial running through 2029. TRIUMPH-1 is the one that anchors the obesity claim.
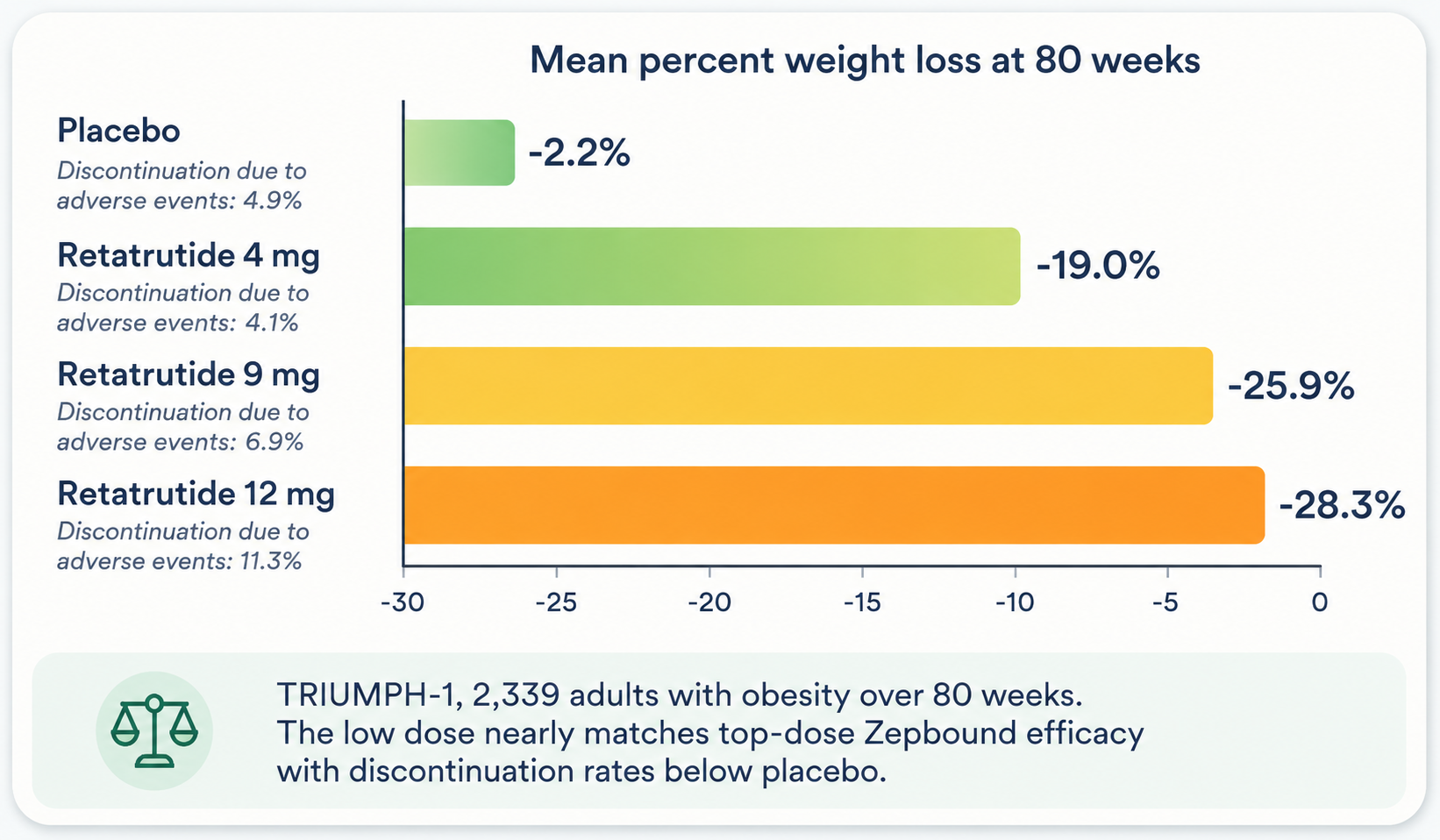
The trial randomized 2,339 adults with obesity or overweight (no diabetes) to one of four arms in a 1:1:1:1 ratio: retatrutide at 4 mg, 9 mg, or 12 mg weekly, or placebo. Treatment ran for 80 weeks. Like Zepbound and Wegovy, the drug is given as a once-weekly subcutaneous injection, with the dose gradually escalated to minimize gastrointestinal side effects.
The primary endpoint is percent change in body weight at 80 weeks. The headline number under the efficacy estimand (the analysis that excludes data after treatment discontinuation, the way most obesity trial headlines are reported) is 28.3 percent weight loss at the highest 12 mg dose, against 2.2 percent in the placebo arm. The 9 mg arm came in at 25.9 percent. The 4 mg arm came in at 19.0 percent. The conservative treatment-regimen estimand, which is closer to an intent-to-treat analysis and includes everyone regardless of whether they finished, is lower across the board: 25.0 percent at 12 mg, 23.7 percent at 9 mg, 17.6 percent at 4 mg. Both estimands matter. The efficacy estimand tells you what the drug can do in patients who tolerate it. The treatment-regimen estimand tells you what happens in the real population that takes it.
For context, the same kind of head-to-head numbers for the FDA-approved alternatives sit around: Zepbound (tirzepatide) at top dose lands at 20 to 22 percent body weight loss at 72 weeks. Wegovy (semaglutide) at top dose lands at about 15 percent at 68 weeks. The pill versions of both drugs come in at 12 to 14 percent. Retatrutide at top dose is roughly a 6 to 8 percentage point step above Zepbound, and 13 to 16 points above Wegovy.
The subgroup analysis matters more than the topline. In patients with BMI ≥35 (moderate to severe obesity) followed for the full two years of the extension period, the top dose produced 30.3 percent weight loss, or 85 pounds on average. That is the gastric-bypass-equivalent number. Roughly 65 percent of patients on the 12 mg dose ended the trial below a BMI of 30 (no longer obese by category). 37.5 percent of patients who started with class-3 obesity (BMI ≥40) ended below BMI 30. Forty-five percent of patients on 12 mg achieved at least a 30 percent weight loss. 27 percent achieved at least 35 percent.
The cardiometabolic secondary endpoints all moved in the right direction. Waist circumference dropped by 9.5 inches at the top dose against 1.4 inches on placebo. Non-HDL cholesterol came down. Triglycerides came down. Systolic blood pressure came down. High-sensitivity C-reactive protein came down. None of these surprised anyone but all of them strengthen the case for cardiovascular benefit, which is the indication the broader CV outcomes trial is designed to formally test.
Then there is the part that gets less coverage and matters more.
The low dose is the real story
Almost every headline about TRIUMPH-1 will lead with the 28.3 percent figure. That is a fair number. But it is not the most interesting number in the trial.
Dan Skovronsky, Lilly’s top scientist, told the New York Times something worth quoting carefully. He pointed out that at the lowest 4 mg dose, retatrutide produced about 19 percent weight loss (which is roughly what people lose on the top dose of Zepbound) while having discontinuation rates due to adverse events that ran 4.1 percent (lower than the placebo arm’s 4.9 percent). In other words, the lowest dose of retatrutide is approximately as effective as the highest dose of Zepbound and seems to be tolerated about the same as placebo. That is a remarkable result. It would normally be the headline, except that the 28.3 percent top-dose figure is louder.
The bodybuilders and biohackers on r/retatrutide have been reporting exactly this pattern for over a year. The sub has 126,000 subscribers as I write this and the top posts of the past month are mostly transformation photos from people running protocols that are far below anything the trial formally tested. The typical dosing on the sub is 0.5 mg to 2 mg per week. That is one-eighth to one-half of TRIUMPH-1’s lowest arm. The results are not subtle. Users routinely report losing 30 to 60 pounds over six to twelve months, sometimes with no GI side effects worth mentioning, often while running other things (TRT, training programs, in some cases growth hormone peptides) in parallel.
What TRIUMPH-1 did today is confirm clinically what those users have been claiming experientially. The dose-response of retatrutide is generous enough that you can run it sub-therapeutically by trial standards and still get meaningful weight loss with minimal side effects. The 4 mg arm of the trial is the closest formal proxy for that experience. The Skovronsky framing in the NYT was Lilly’s first public acknowledgment that the low-dose use case may be the largest commercial opportunity for this drug, larger than the severely obese subgroup that gets the 30 percent loss at top dose.
This is the part of the story that explains why retatrutide is going to be a bigger drug than tirzepatide. The obesity drug regulatory pathway is optimized for severely obese patients (BMI ≥30, often higher) who need to lose large amounts of weight. The trials are designed around that population. The labels target that population. The insurance coverage is built around that population. But the actual demand extends well beyond it. There are tens of millions of Americans with a BMI in the 25-to-30 range who want to lose 15 to 30 pounds, for reasons that include cardiovascular risk reduction, aesthetic preference, joint loading, sleep apnea, or simply feeling better in their bodies. For that population, top-dose Zepbound is overkill and top-dose retatrutide will be more so. Low-dose retatrutide may be exactly the right tool. The gray-market users figured this out empirically, well before today’s trial readout.
The dose-response in TRIUMPH-1 also shows the cost of going to the top dose. At 9 mg, weight loss is 25.9 percent and discontinuations due to side effects are 6.9 percent. At 12 mg, weight loss is 28.3 percent and discontinuations are 11.3 percent. You buy approximately 2.4 additional percentage points of weight loss for roughly a doubling of dropout rate. For severely obese patients with high-risk profiles, that trade is worth it. For the much larger population of moderately overweight adults looking for a 15-to-20-pound recomposition, the lowest dose (and possibly less than that, based on what the r/retatrutide community is doing) is the right call. The 4 mg arm is the conservative anchor. The 9 mg arm is the sweet spot for harder cases. The 12 mg arm is for severe obesity.
The caveat to all of this is that nothing below 4 mg has been formally tested in a Phase 3 obesity trial. The r/retatrutide protocols at 0.5 to 2 mg are empirical, not clinical. They lack the safety surveillance, the standardized titration, the lab monitoring, and the placebo control that the trial provides. If the trend holds (and Lilly’s published Phase 2 dose-ranging data suggests it does, including doses as low as 1 mg producing meaningful weight loss above placebo at 48 weeks), then the eventual label will probably support starting doses well below 4 mg, especially for non-obese patients. The clinical Phase 3 confirmation of the very-low-dose use case is something Lilly will have to do later, probably as a post-approval label expansion. The casual users have already done the unofficial version.
One new side effect worth knowing about
The side effects at the top dose track what you would expect from a more potent incretin agonist: more nausea (42 percent at 12 mg vs 15 percent on placebo), more vomiting (25 percent vs 5 percent), more diarrhea, more constipation. None of those are new to anyone who has been on Zepbound or Wegovy. They scale with dose.
The one signal worth flagging that does not show up the same way in the tirzepatide trials is dysesthesia. Twelve and a half percent of patients on the top retatrutide dose reported abnormal skin sensations (tingling, burning, numbness) compared to less than one percent on placebo. This is likely related to the glucagon receptor agonism, which is unique to retatrutide in this class. It is not necessarily a deal-breaker (many of these events resolved or were mild) but it is going to be on the label and it will be a real consideration for some patients. The 4 mg dose had dysesthesia in 5.1 percent of patients (still elevated against the 0.9 percent placebo rate, but much lower than the top dose).
Why three hormones might beat two
Retatrutide is a synthetic peptide that activates three different gut-hormone receptors at once: GLP-1, GIP, and glucagon. To understand why this is a big deal, it helps to look at how the obesity drug class has built up over the past decade.
The first generation was the GLP-1 agonists alone. Liraglutide came first, then semaglutide (Ozempic for diabetes, Wegovy for obesity). They mimic the action of glucagon-like peptide-1, a gut hormone released after meals that does several things: it tells the pancreas to release more insulin, it tells the stomach to empty more slowly, and it tells the brain you are full. Top-dose semaglutide produces about 15 percent body weight loss in obesity trials.
The second generation added a second receptor, GIP (glucose-dependent insulinotropic polypeptide), which is another incretin hormone with overlapping but distinct effects. Tirzepatide (Mounjaro for diabetes, Zepbound for obesity) hits both GLP-1 and GIP. The combination produces about 20 to 22 percent weight loss at top dose, roughly a one-third increment over semaglutide. Nobody fully understands why adding GIP to GLP-1 makes the package more effective, but the leading hypothesis is that GIP modulates appetite and energy balance through pathways the GLP-1 receptor doesn’t reach.
Retatrutide is the third generation. It hits GLP-1, GIP, and glucagon. Glucagon is the metabolic counter-hormone to insulin, and it has been hard to develop drugs that target the glucagon receptor without raising blood sugar. The pharmacology of retatrutide solves this by tuning the relative receptor activities such that the glucagon component increases energy expenditure, promotes fat breakdown, and modulates hepatic glucose production, without breaking blood sugar control because the GLP-1 and GIP components compensate.
The why is partly biology and partly empirical. We do not have a complete mechanistic story for the additional weight loss. We can see in the data that the three-receptor package produces more weight loss than the two-receptor package, which produces more than the one-receptor package, and the side-effect cost scales sub-linearly. There may eventually be four-receptor or five-receptor combinations. Lilly’s pipeline already includes a few. None of them have read out yet at the Phase 3 scale.
The practical implication for you, the reader, is that this drug class has not finished evolving. Anyone telling you “this is the final answer” is wrong. Retatrutide is one step on a curve that is still going. Five years from now there will probably be something better. That does not mean today’s drugs aren’t worth taking. It means the longer-term commitment is to the class, not to any one molecule.
The peptide black market got there first
Here is the part of the story you will not see in the New York Times.
For more than a year before today’s TRIUMPH-1 readout, retatrutide has been freely available in the United States through a network of “research peptide” retailers. These companies sell synthesized peptides labeled “for research use only” (RUO), which is a legal carve-out that lets them ship compounds without the FDA-regulated drug pathway, on the theory that the buyers are research labs or independent scientists running experiments on cell cultures or animals.
In practice, the buyers are bodybuilders, biohackers, men and women in their thirties through fifties who want a 20-to-40-pound cut without insurance friction, and a smaller group of people who cannot afford or cannot access the FDA-approved alternatives. The forums where they congregate (r/retatrutide with 126,000 subscribers, r/Peptides, several Telegram groups, and a layer of private forums) have been openly discussing retatrutide protocols since at least early 2024. Threads with titles like “RETA 8 weeks in, down 22 pounds” predate today’s Lilly press release by more than a year. There are people who have completed twelve-month cycles of retatrutide before the Phase 3 trial finished enrolling.
The dosing on r/retatrutide is the interesting part. Users typically start at 0.5 mg per week and titrate up to 1 mg or 2 mg, holding there. That is well below the 4 mg lowest-tested arm of TRIUMPH-1. The community has effectively run a large uncontrolled experiment showing that retatrutide produces meaningful weight loss at doses Lilly never formally tested in a Phase 3 trial. The transformation posts are consistent: 30 to 60 pounds over six to twelve months, often with mild or no GI side effects, sometimes paired with TRT or training programs. The dysesthesia signal that hit 12.5 percent at the 12 mg trial dose appears much rarer in the r/retatrutide reports, which is consistent with the trial’s own dose-response (5.1 percent at 4 mg, presumably lower still at sub-4 mg doses, though we do not have controlled data at those doses).
What this means for the regulatory and commercial story is significant. The casual user (someone who wants a 15-to-25-pound recomposition, not someone with severe obesity) has found that retatrutide at one-quarter to one-half of the trial’s lowest dose produces results comparable to a top-dose Zepbound prescription, with better tolerability and lower cost. The gray market has been running the use case that Lilly’s regulatory pathway has not yet formally validated. The TRIUMPH-1 data, by showing that even the 4 mg arm produces 19 percent weight loss with sub-placebo discontinuation rates, makes the very-low-dose use case plausible to anyone reading the trial carefully. The r/retatrutide community has been making this argument with photos and protocols for a year.
The supply comes from two main places. The first is American “peptide companies” that operate in a legal gray zone, selling RUO-labeled vials with disclaimers that nobody reads. The second is direct-from-China factories that ship to US addresses, sometimes through US-based reshippers, sometimes directly. The Chinese factories are the actual source for most of the supply chain; the American resellers are repackagers.
What you are buying when you order retatrutide from these channels is can be highly variable. Some products test out at 80 to 95 percent pure on third-party HPLC analysis. Some test at 50 percent. Some have the wrong peptide entirely. Some have residual solvents, heavy metals, or bacterial endotoxins from inadequate purification. Dosing is improvised. The vials come with reconstitution instructions written for people who already know how to work with peptides, and protocols are shared on forums rather than prescribed by clinicians. Nobody is running your labs. Nobody is monitoring you for the dysesthesia signal. Nobody is titrating your dose based on tolerability or your goals.
To say this clearly: the harm-reduction picture for the gray-market retatrutide market is bad. Compounded tirzepatide from FDA-registered 503A/503B compounding pharmacies (which is its own very murky landscape but at least one with some US regulatory oversight) is not the same thing as RUO peptide from a Chinese chemical factory. The compounding pharmacy market exists because tirzepatide was on the FDA drug-shortage list, which made it legal for compounders to produce. Retatrutide is not FDA-approved at all, so there is no shortage and no legal basis for compounding. Anyone selling retatrutide in the US right now is, regardless of how their website is worded, operating outside the drug regulatory framework.
I am writing this from the perspective of someone who has been on Zepbound for eighteen months, who has watched the compounded-tirzepatide market mature, and who has had several conversations with men in their forties and fifties who are considering the RUO retatrutide route because they are either uninsured for Zepbound or unwilling to wait the two to three years for retatrutide to be FDA-approved. I understand the temptation. The drug works. The TRIUMPH-1 data, now public, confirms that the drug works. The legitimate version is over a year away. FOMO is real.
But I am also going to be direct: if you go that route, you are running an N-of-1 experiment on yourself with a compound of unknown purity, no medical supervision, no titration support, and no liability if something goes sideways. The most likely outcomes are fine. Some people will lose seventy pounds and have no problems. Some will get the GI side effects and stop. A smaller number will run into the dysesthesia (which the TRIUMPH-1 data shows is real and dose-dependent and probably underrecognized in the gray market). A smaller number still will have a bad batch with a contaminant and end up in an emergency room. The base rate of bad outcomes from gray-market peptides is not catastrophic but it is not zero, and it is not what you would get from an FDA-approved version through a real clinic.
The honest harm-reduction advice if you are going to do this anyway: third-party-test your vials through a service like Janoshik or similar, start at the lowest dose, titrate slowly, get your labs done independently, and have a clinician you can talk to even if they are not prescribing. None of this turns gray-market retatrutide into FDA-approved retatrutide. It just reduces the downside.
For the median reader of this post, the right move is not to chase it. The legitimate version is coming. The wait will be hard for people in the worst shape and easier for people in better shape. I am writing the rest of the post for the wait.
When you will actually be able to get it (legally)
The TRIUMPH program has four Phase 3 trials in addition to dedicated trials for cardiovascular outcomes and the head-to-head retatrutide-vs-tirzepatide study. Today’s TRIUMPH-1 readout is the obesity registrational trial. The other key readouts are still ahead.
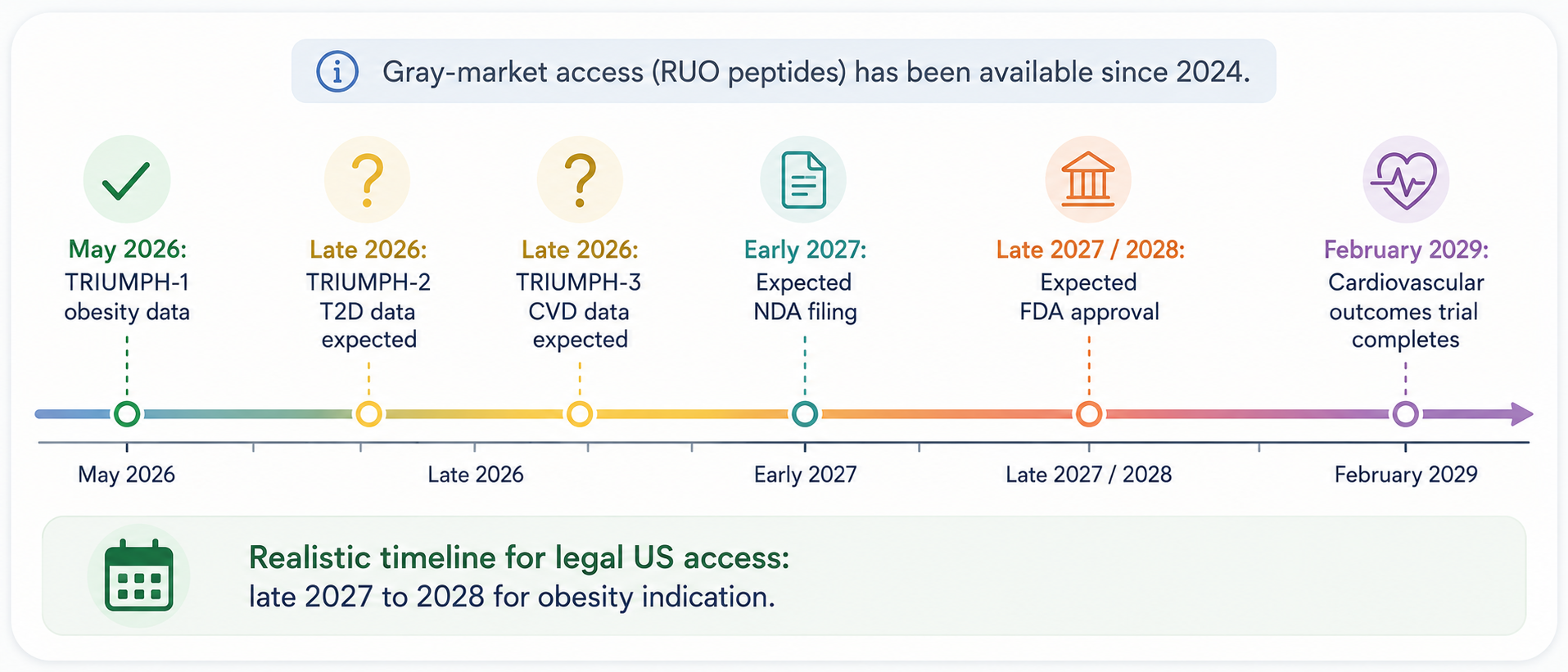
TRIUMPH-2 covers the type 2 diabetes population, with the basket-trial structure that also includes obstructive sleep apnea and knee osteoarthritis protocols. Topline data is expected “later this year” per Lilly’s release, which most analysts read as the second half of 2026.
TRIUMPH-3 covers patients with established cardiovascular disease who also have obesity, a population that is particularly relevant for the broader cardiovascular indication. Topline data is also expected later this year.
TRIUMPH-4 is the stand-alone knee osteoarthritis trial. Lower priority for the regulatory filing but matters for the broader label.
The dedicated cardiovascular and kidney outcomes trial in adults with obesity (TRIUMPH-Outcomes / NCT06383390, 10,000-patient enrollment, populations with established atherosclerotic cardiovascular disease or chronic kidney disease) does not complete its primary endpoint until February 2029. That trial is what would support a formal cardiovascular-risk-reduction claim, which is what made Wegovy and Zepbound their broader markets.
Putting the pieces together: Lilly will likely file the New Drug Application (NDA) for retatrutide for obesity in late 2026 or early 2027, after they have TRIUMPH-1 and TRIUMPH-2 data in hand. FDA review of a novel obesity drug typically takes about ten months under standard review or six months under Priority Review (which obesity drugs sometimes qualify for under the Subpart H accelerated approval framework, though Lilly has not signaled that this is the path). Realistic obesity approval is late 2027 or 2028.
For context, tirzepatide had its T2D approval (Mounjaro) in May 2022 and its obesity approval (Zepbound) in November 2023, roughly eighteen months apart. Retatrutide is on a similar arc but lagging by about three years.
One additional commercial wrinkle worth knowing about: Lilly has been in court with the FDA since 2024 trying to get retatrutide reclassified as a biologic rather than a traditional drug. The fight hinges on a technical question about how many amino acids the molecule contains. Biologic status would mean longer market exclusivity (twelve years for biologics vs five years for new chemical entities) and would block competitor generics or biosimilars for that much longer. The NYT estimates the difference is worth billions of dollars to Lilly. The case is still tied up in court. The outcome will affect how aggressively Lilly prices retatrutide and how long it takes for cheaper alternatives to come to market.
The compounding pharmacy landscape is its own dimension. If Lilly maintains FDA-approved supply at launch (which they will work hard to do, based on the lessons learned from tirzepatide’s shortage period in 2023-2024), the drug should not go on the FDA shortage list, and the compounding pharmacies that have been the cheaper-tier supply for tirzepatide will not be able to compound retatrutide legally. That removes one of the routes by which people without insurance currently access GLP-1 drugs. The implication: retatrutide will be expensive at launch and accessible primarily through commercial insurance.
What to do today if you are on a GLP-1
Four groups of readers, four different answers.
If you are currently on Zepbound, Mounjaro, or Wegovy and it is working: do not change anything based on today’s news. The drug you are on is real, FDA-approved, monitored, covered (at least partially) by your insurance, and producing meaningful weight loss for most people. Retatrutide is not available legally. The gray-market route has real downsides. The right move is to stay on what you are on, get your labs done at the cadence your doctor recommends, and check back when there is something concrete to switch to. That moment is probably late 2027.
If your current GLP-1 is working but the side effects are wearing you down, retatrutide does not solve that problem yet. The 12 mg dose of retatrutide has worse GI tolerability than Zepbound. The interesting result from TRIUMPH-1 is that the 4 mg low dose of retatrutide may eventually offer Zepbound-equivalent results with much better tolerability, but that is two to three years away from being available to you. For now, the conversation with your doctor about tolerability is still the standard one: dose adjustment, slower titration, anti-nausea support, or in some cases a switch within the existing approved class.
If you are severely obese (BMI ≥35) and have been on a GLP-1 with submaximal results, retatrutide is the drug to watch. The bariatric-equivalent weight loss in the BMI ≥35 subgroup of TRIUMPH-1 is the most distinctive part of the trial. If you have been struggling to lose enough weight on Zepbound or Wegovy and the gap is what gets you to a healthy BMI, retatrutide may eventually be the answer. The honest framing of your timeline: keep losing whatever you can lose on your current regimen, work on cardiometabolic markers and resistance training in the meantime, and plan to revisit the decision in 2027 when the legitimate version is closer.
If you are not on any GLP-1 today and are considering one for the first time, retatrutide does not change your decision. Start the conversation with your doctor about Zepbound or Wegovy now. Get the labs done. Get the prior authorization done. Get on what is available. By the time you would be ready to plateau on your initial drug, the next one will be either approved or imminent. That is the right sequencing.
If your BMI is between 25 and 30 and you want a 15-to-25-pound recomposition, you are the demographic the gray market is built for, and the legal pathway is hardest for you. This is the honest answer. FDA labels for the existing obesity drugs require either BMI ≥30 or BMI ≥27 with a weight-related comorbidity (diabetes, hypertension, sleep apnea, dyslipidemia). The retatrutide label, when it lands, will almost certainly use the same threshold. Insurance coverage is even tighter than the label. The casual recomposition use case (the “I want to look better in a Mediterranean linen shirt this summer” use case) is not what these drugs are marketed for, and your doctor probably will not prescribe at the gentle dose you actually want. The options you have are: pay out of pocket via LillyDirect for Zepbound at around $349 to $499 per month for vial pricing (if a prescriber will write for you), find a telehealth service that will prescribe more flexibly, or go gray-market with all the caveats from the prior section. The reason r/retatrutide has 126,000 subscribers and is growing is that this category of user has not had a clean legitimate option. That may not change for another three to five years, when post-approval label expansions could open the door to lower-BMI use cases. In the meantime, the legitimate-route advice is: do the work on training and diet first, recognize that 15 pounds of body recomposition is achievable without pharmacology in most cases, and if you decide the gray-market route is worth it, apply the harm-reduction checklist from the prior section.
For all four groups, the gray-market peptide question is the same: probably not worth it for the median person. The legitimate timeline is real. Today’s TRIUMPH-1 readout, far from being a reason to chase RUO peptides, is actually the reason to wait. The trial worked. The drug is real. The FDA approval is on a known timeline. The cost of waiting is eighteen to thirty months of staying on whatever is working for you now. The cost of not waiting is running an experiment on yourself with a compound nobody has audited and no clinician will help you manage. The math has rarely been clearer.
I am going to stay on Zepbound at my current dose, watch the TRIUMPH-2 and TRIUMPH-3 readouts later this year, and have a real conversation with my doctor at Marek Health when retatrutide is actually available through a legal pharmacy. The drug that may eventually replace what I am on is real. It is just not real yet for me. The discipline of the next two years is the same discipline that got me here in the first place: trust the data, stay on the protocol that is working, do not improvise based on what is on a forum.
I keep a running tracker of every GLP-1 and incretin drug, approved and still in the pipeline, with what each one targets, how far along it is, and what's coming next.
See the full GLP-1 Pipeline Tracker →About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.