
The years I stopped moving
Get the free Bloodwork Decoder
Testosterone is one number worth understanding. So are the dozen others on your panel. I put them all on a one-page cheat sheet: what each means, what to aim for at 50, and what to ask your doctor. Subscribe free and I’ll send it over. No spam, nothing to sell.
I worked through most of the pandemic in our small, dark guest room, which was normally my mother-in-law’s room when she came to visit. I was hunched over on a couch staring at a laptop. The day often started early and ended late because a lot of my work was on video calls with people in California (three hours behind me), Spain (six hours ahead), and China (twelve hours ahead, give or take). Our older son had just started preschool and our younger had just learned to walk. My wife was homeschooling the four-year-old through preschool and the first year of school which was incredibly hard on everyone.
I stopped moving and I do not mean didn’t exercise. I mean I stopped moving in any meaningful way that wasn’t getting up to refill the coffee. I gained a lot of weight and I was not weighing myself.
The thing that somehow became routine, that my wife noticed and did not comment on, was eating a pint of Ben & Jerry’s most evenings in bed after the kids were asleep. She later told me she didn’t say anything because it seemed like the only thing I enjoyed somewhat. That sentence still haunts me when I think about it now.
What I’m describing is obviously depression, but I would not have called it that at the time. I had always had a fair amount of anxiety. Through the pandemic the anxiety started bringing depression along with it. I was tired in a way that did not respond to sleep. I had very little patience with my kids, which is a thing you only realize is a problem when you watch yourself snap at a five-year-old for something silly and then catch the look on the five-year-old’s face. My libido was non-existent. Most days felt like a never ending grind. I was only hanging on to keep paying for a life I was not enjoying. I would sit in the guest room and try to work out how many years I had to keep doing this before I could stop and retire. The answer was always somewhere north of ten.
In February 2021 I made an appointment with a psychiatrist. I was diagnosed with generalized anxiety disorder and depression. I have been seeing one ever since.
The medication helped. It smoothed out the real lows but my average mood was still pretty low. I was a little less anxious about work and less ground down by the worst days, but the way I felt did not change in any way I would have called a recovery. The fatigue stayed, the libido was still zero, and I still had very little patience with my kids in the late afternoon. The weight kept climbing. I was not weighing myself for the same reason I was not getting physicals. I did not want to see the number, and I did not want to hear all the things wrong with me either. I am genuinely shocked now when I look at photos of myself from this period. I have no memory of being that big, which I think is part of how it happens.

373 pounds and a self-pay testosterone test
The decision to actually go see a doctor was not really mine. My wife made it. At some point in 2024 she decided that we were both adults and, more importantly, parents, and that adults and parents had regular physicals. Neither of us had one in years. She found a PCP who would take new patients, accepted the six-month wait, and put us both on the calendar. She was probably worried about my health but was not saying so out loud. That was already more than I deserved.
The appointment came in October. I weighed 373 pounds, which terrified me. I made the decision to change sitting on the exam table while the nurse went to get the doctor. Seeing the number, the actual number, on the scale, made something move in me. I called it intuitive at the time and I would still call it that. There was no plan, just a decision that I had to start taking care of my health that week.
My PCP put me on Zepbound, which I had been wondering about and considered an option. That evening I started learning everything I could about weight loss, nutrition, training, and metabolic health. Being an engineer means I do not know how to take an interest in something without trying to understand everything about it. I was reading papers, listening to podcasts in the car and in bed, and watching YouTube channels I would not have known existed eight weeks before. Low testosterone came up in this exploration quite a bit and the more I read, the more I realize the description of symptoms sounded very much like what I was experiencing.
I was hesitant at first, because I felt messing with hormones and injecting steroids was something that people with serious physical conditions or body builders did. However, I am a scientist at heart, so decide to measure. I ordered a self-pay testosterone test through Labcorp. This was something I had learned about in the same learning journey. You do not have to wait for a doctor to order it, you can go to Labcorp’s or Quest’s website, pay out of pocket, and have the blood drawn that week. The result came back at 230 ng/dL. The reference range starts at 264. I was below that floor.
I am not a clinician but the number seemed straightforward enough to read. I had a bunch of symptoms that matched low testosterone and a number that confirmed it. I talked to my wife. She obviously knew that I was miserable. We agreed I should pursue TRT.
The question was where to go. My PCP could prescribe testosterone, but the standard primary care workflow for hypogonadism seems not where careful investigation happens and to be honest I was too embarrassed to have that discussion with her at that point. I was listening to a guy named Derek, whose YouTube channel is called More Plates More Dates. He is an unusual figure. He has a substantial following in the lifting and physique community and he is also unusually well-informed on the science of hormones, peptides, and the supplement industry. The standard caveats about following YouTube health figures all apply. I had watched dozens of hours of his content by this point and I had calibrated where his analysis seemed sharp and where it seemed to lean into “meathead on gear” logic. He founded a telehealth clinic called Marek Health. They specialize in the kinds of hormonal workups that primary care does not always do well. I signed up.
I realize the idealized version of this story would have me arriving at a urologist or endocrinologist through some pristine evidence-only channel. The honest version is that I went there because the YouTuber I had been learning from founded it. The reason I am willing to write that out loud is that the trust came first. I had spent dozens of hours assessing his reasoning and trustworthiness before I decided to send any money to a clinic he founded. They seemed to have a solid reputation and be more thorough than the average “pill mill” TRT clinic.
The Marek protocol, and what it did for me
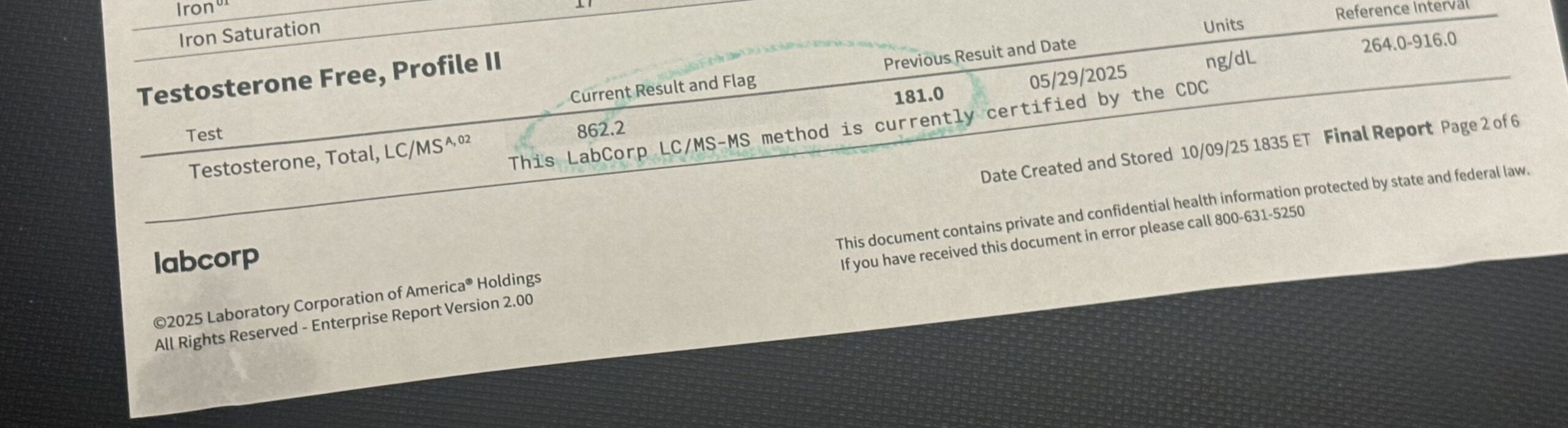
The Marek intake was thorough. They ordered a full panel including a confirmatory testosterone test, a complete metabolic and lipid workup, sex hormone binding globulin, free testosterone, LH, FSH, estradiol, hematocrit, hemoglobin, DHEA-S, PSA, and a whole lot of markers I had to look up. The follow-up testosterone reading was 181 ng/dL. Two readings, both well below the reference range, were enough to confirm I was hypogonadal.
The protocol they prescribed was testosterone cypionate, 120 mg per week, split into three subcutaneous injections. I have since learned this is a good protocol; splitting the weekly dose into three smaller injections produces more consistent blood testosterone levels day to day than the older once-weekly intramuscular approach. The injection itself was not something I was worried about. I had been injecting Zepbound for months at that point, and as a teenager I had spent six years getting weekly allergy shots.
They also prescribed a supporting panel: DHEA, Pregnenolone, Tadalafil 5 mg daily, and Homocysteine Supreme (a B-vitamin formulation, because my homocysteine had come back at 17.9, well above the 10-or-below range that you want). This is the part of the experience I had been most worried about. The concern with telehealth TRT clinics is that they ride the prescription you actually need into selling you supplements you may or may not need. Marek did some of this, but the items they recommended seemed not random. DHEA and Pregnenolone are both upstream of testosterone synthesis and there is at least some clinical evidence they can support hormonal balance in older men. Tadalafil is a PDE5 inhibitor approved for both erectile dysfunction and benign prostatic hyperplasia, and there is reasonable evidence that low daily dosing benefits both endothelial function and prostate health. Homocysteine Supreme was a real intervention for an actually-elevated lab value.
What I ended up doing over the months that followed was triaging each item by whether it helped and whether the source mattered. The testosterone, DHEA, and Pregnenolone are hormonally active and I wanted them through a clinic that does ongoing monitoring of the relevant labs. Those stayed with Marek. The Tadalafil is a generic prescription drug. My PCP writes it for me now through insurance, at a fraction of the price. The Homocysteine Supreme is an off-the-shelf supplement that I buy from any reputable seller. I am still a happy Marek customer for the things that need a clinic.
The first thing that came back was libido. I do not have a precise date for it because I was not tracking the way I was tracking weight, but somewhere in the first three or four weeks I noticed I was feeling like a teenager — luckily things stabilized at a more reasonable level after a few months.
The mood and energy changes came in slower, over months. Some of this was because of testosterone and some of it was because of Zepbound and the weight I was now visibly losing and the trainer I had also hired right around this time. I cannot tell you what fraction of the mood lift came from which intervention, and anyone telling you they can perform that decomposition on themselves is lying.
What I can tell you is that by late summer 2025 I was a different person in ways my wife and kids noticed. I could move. I had patience again. The late-afternoon energy crashes stopped, and at the end of a workday I did not feel like the day had wrung me out.
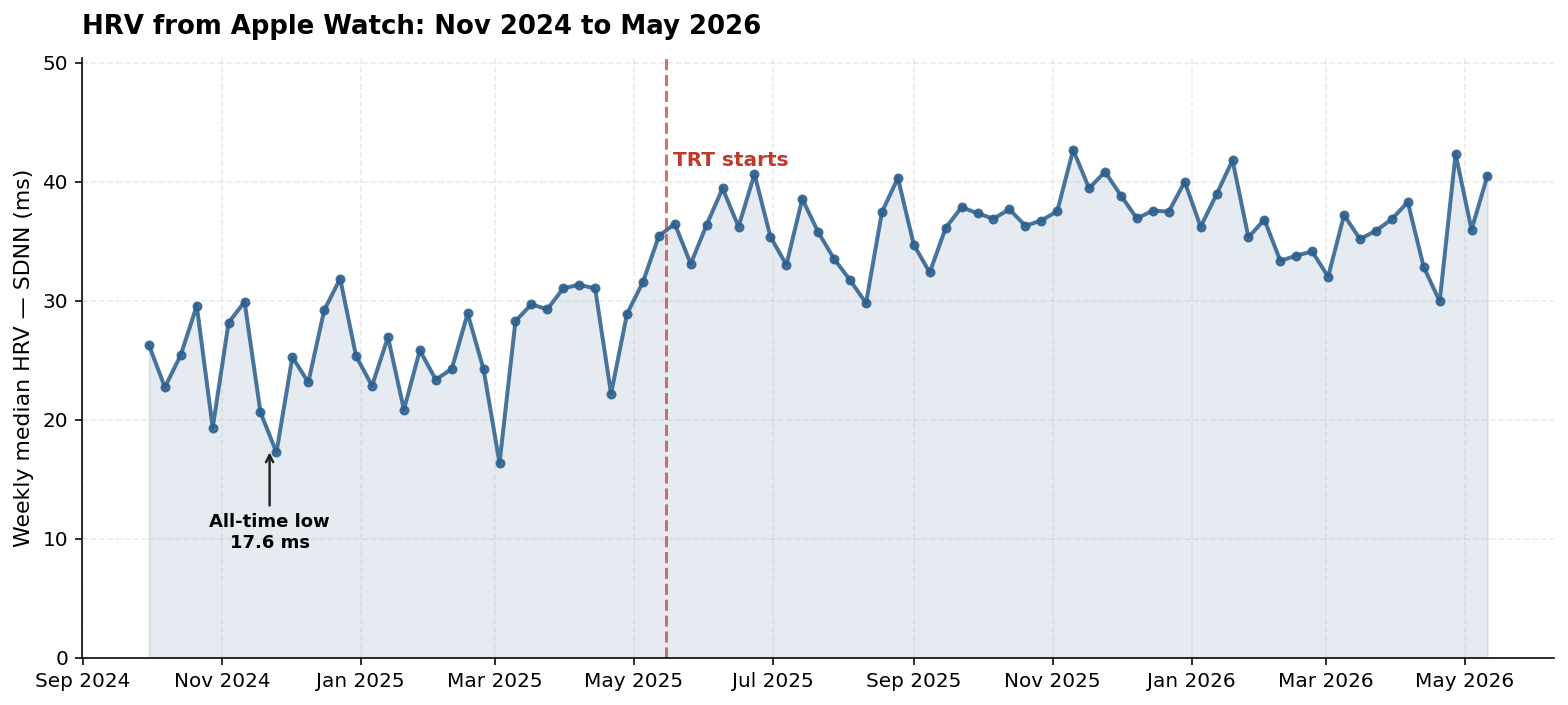
The numbers caught up to what I was feeling. By October 2025, five months in, my total testosterone was 862 ng/dL, well into the high-normal range. My HRV, which had been at 17.6 ms in November 2024 (a number my Apple Watch describes as “severely stressed”), had climbed into the 40s, with a personal peak of 51.3 ms a few weeks later. My resting heart rate had dropped from around 80 bpm to the mid-60s and would later settle in the low 60s.
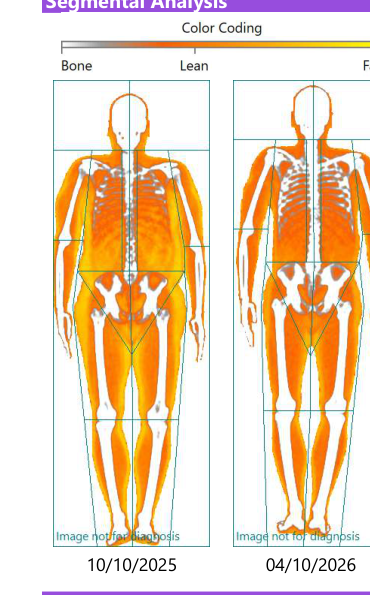
The body composition change is the part that surprised me the most, especially since everyone talks about folks on GLP-1s losing tons of muscle. In April 2026 I had a DEXA scan that showed I had lost 44 pounds of fat and gained 9.6 pounds of lean mass over the previous six months. Losing fat and gaining muscle in a caloric deficit is hard! It usually requires three things working together: testosterone, progressive resistance training, and adequate protein intake. I had all three at the right doses for the first time in my adult life.
A week after the DEXA I had a resting metabolic rate test (indirect calorimetry, the test where you breathe into a mask for 10 minutes while chilling in a comfy recliner), which showed my RMR was 10% above what the standard prediction equations would have estimated from my body composition. This was not what should happen after losing 170 pounds. The expected outcome is metabolic adaptation, where your body burns fewer calories than predicted as a defense against further weight loss. Mine had gone the other way, and the most plausible reason is that testosterone increases the metabolic rate of lean tissue, and I had spent the previous five months adding lean tissue.
The risks I was looking out for
I looked out for the things you read to be worried about. The big four are polycythemia (your blood thickening up because testosterone tells your bone marrow to make more red blood cells), prostate trouble (TRT was contraindicated for prostate cancer survivors until pretty recently), estradiol overshooting because the body aromatizes some testosterone into estrogen, and fertility going down because exogenous testosterone shuts off the signals that tell your testes to keep making sperm. The honest summary on each is short.
Hematocrit. Mine climbed from 41.9% pre-TRT to a peak of 49.7% five months in, and has since settled back to 47.5%. The threshold most clinicians watch for is 51% to 54%, above which the standard intervention is a therapeutic phlebotomy (a regular blood donation, essentially) to thin things out. I never crossed the threshold. The settle-back is probably explained by the weight loss, hydration, and the fact that hematocrit climbs early on TRT and then stabilizes.
Prostate. My PSA has been 0.3 to 0.5 ng/mL across all my visits, with a free-PSA percentage of 50% at the most recent test, which is the favorable side of the ratio. The clinical default not many years ago was that TRT in a patient with elevated PSA or a prostate cancer history was unacceptable. A trial from this May out of JAMA Internal Medicine, Bhasin and Burnett and colleagues, formalized what endocrinologists who watch this literature have been saying for years: TRT in carefully selected prostate cancer survivors with hypogonadal symptoms does not increase recurrence. The clinical evidence has been catching up to people like me.
Estradiol. The manosphere position on estradiol in men on TRT is that you should crush it down with an aromatase inhibitor. The Endocrine Society position is the opposite, which is that estradiol in the normal-to-mid-range is protective for bone density, cardiovascular health, and mood in men, and that aromatase inhibitors are over-prescribed. My estradiol has stayed in range throughout, sometimes just into the high end. I have never taken an AI and Marek has never suggested one.
Fertility. Exogenous testosterone shuts off LH and FSH, which are the pituitary signals that tell the testes to make sperm. On my labs, both LH and FSH are in fact down to 0.2 to 0.3 (well below the floor of the reference range), which is exactly what you would expect on TRT and confirms the protocol is doing what it does. This is not a problem in my particular case because my wife and I have two kids by adoption and are not planning to have more biologically. For a younger man, or for a man still hoping to have biological children, fertility preservation on TRT is its own substantive conversation involving HCG, clomid, or stopping TRT entirely. I am not the right person to write about that. Talk to your doctor.
The TRT conversation that does not sound the same
There is a cultural moment around testosterone right now that has very little to do with hormone replacement and a great deal to do with politics, cosplay, and a particular flavor of online masculinity grift. The current US Health Secretary is part of a political coalition that treats testosterone as a coded masculinity signal. The manosphere has built an entire content economy around it, selling teenagers supplement protocols designed for 50-year-olds and explaining that seed oils, vaccines, and modern medicine in general are what made your father weak. The conversation has been collapsed into a stage prop for the red-pill / MAHA / “alpha male” economy, and the people in that space do not actually care whether you are hypogonadal.
I am not a UFC fighter or interested in “mogging” anyone. I take testosterone because my body stopped making enough of it on its own, and the absence of it was making me less of a parent, less of a partner, and less able to do the work I was being paid to do. None of that has anything to do with the cosplay.
There are two TRT conversations happening at once and they only sound the same. One is medical: a measurable hormone deficiency in middle-aged men, the clinical workup that confirms it, the dose that corrects it, the labs that monitor it, and the research that has been catching up to it. That conversation has its own caveats and an active literature. The other conversation is about testosterone as identity, as posture, as part of a kit of beliefs about who men are supposed to be. The political version is loud, and it is making it harder for the medical version to be heard in the rooms where it matters. Most of the men I know who would benefit from a careful evaluation for hypogonadism are not going to ask their doctor about it because they do not want to be associated with the loud version.
The clinical guidelines have been moving over the past several years. The cardiovascular safety question, which scared a generation of doctors away from prescribing TRT, was substantially answered by the TRAVERSE trial in 2023. The prostate cancer survivor question is the one the Bhasin paper from this May addressed. On estradiol, the Endocrine Society has been pushing back on the over-prescription of aromatase inhibitors. The picture, slowly, is becoming what the evidence has been saying for years. The picture in the popular discourse is going the other direction.
I have been on the same protocol for a year now: 120 mg of testosterone cypionate per week, split into three subcutaneous injections, with regular monitoring labs through Marek. My most recent panel showed total testosterone at 860 ng/dL and the other relevant markers in good shape. Body weight is steady around 205 pounds, down from 373. My lipid panel looks great even under the new, aggressive 2026 guidelines. The version of me that was sitting in the guest room in 2021 doing retirement math would not recognize this body or this energy or the way the day no longer ends in collapse.
What I would tell that version of myself, if I could, is to get help on the mental health side first, which he did, and then to keep going, because the medication was not going to be the whole answer. The full answer turned out to be a combination that all came together in the same season: Zepbound, a personal trainer, the data discipline of calorie tracking, and TRT. None of them would have worked alone. The thing that made the difference was being willing to actually look at the numbers and try the things the numbers were pointing at.
The men I worry about are not the ones loudly defending their right to take testosterone. They are the ones who would actually benefit from it and will never bring it up with their doctor because they have learned that bringing it up means being mistaken for the loud version.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.