
The food noise went quiet. Then I had to rebuild the rest.
I have thrown out all my clothes twice. Once on the way up, when nothing fit and I kept telling myself the bigger sizes were temporary, and once on the way down, when the bigger sizes were sliding off and I finally let myself believe it. The jeans I wear now are Levi’s 501s in a 36×34, pulled off the rack in the regular section like a normal person. When I started I was in a 46. My T-shirts went from 3XL to L.
I am not telling you this to brag. I am telling you because the scale, 373 pounds down to the low 200s, never quite lands the way a pair of jeans does. Neither does the thing I actually think about on a Tuesday: I no longer dread a coach seat on a work flight, because I fit in it again.
I do not have many pictures from the heaviest part of this. I was too embarrassed to point a camera at myself, which is the same reason I never got a baseline DEXA scan at my top weight, the one comparison I would most want now. The before photo I do have, the orange shirt, I did not even take. My five-year-old grabbed a tablet and snapped it, the way little kids will, and it turned out to be the only honest picture of where I started.

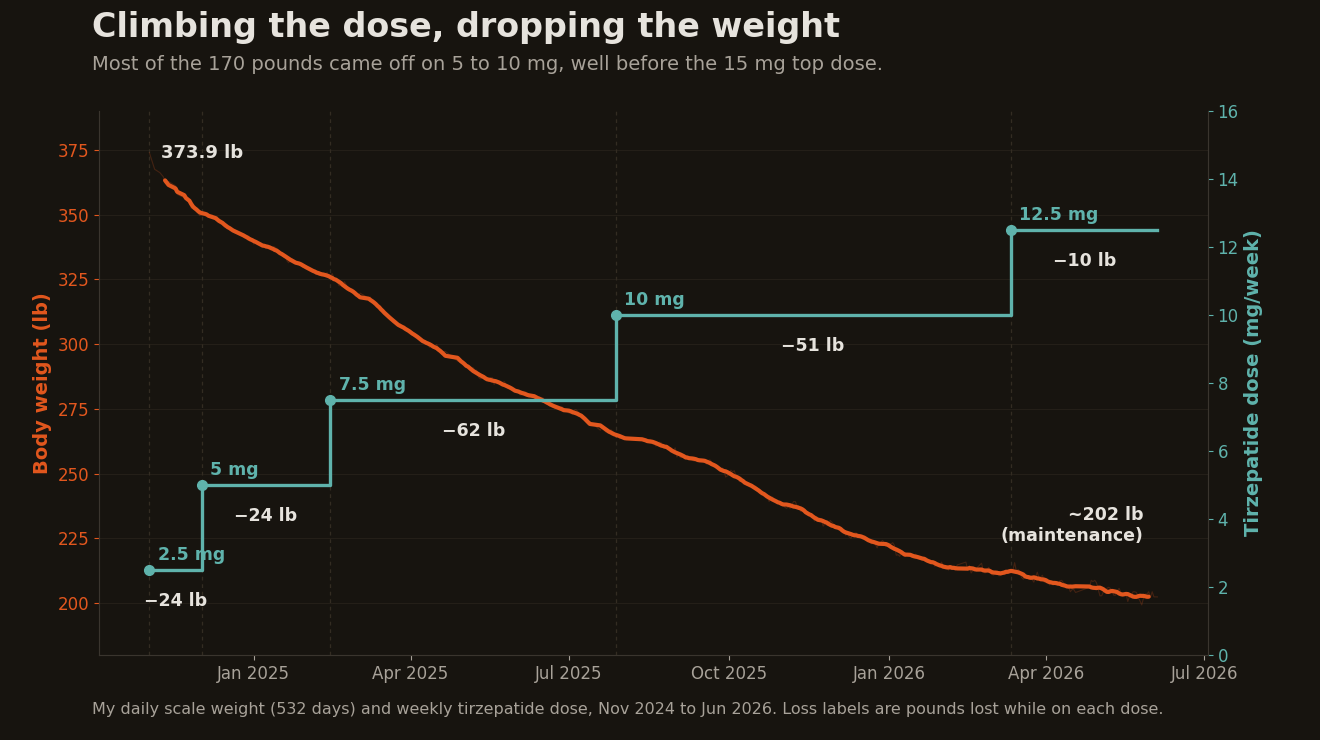
I am 53. Over about eighteen months I lost roughly 170 pounds, a little under half of what I weighed. I did it on tirzepatide, the drug sold as Zepbound, plus a long list of things that were not the drug. This is the honest version of how it happened. What the medication actually did, what it did not do, what surprised me, and why I am still taking it.
One note before the drug names start. This is my personal account, not a protocol. Every medication decision in it, the tirzepatide, the testosterone, the blood pressure and cholesterol pills, was made with my doctors and my own labs in front of us. If you are considering any of them, that is the way to do it.
The drug killed the food noise. The work was everything else.
The most useful thing tirzepatide did was quiet the noise. I did not even understand what food noise was until I tried to diet against it. Early on, when I had started counting and limiting calories but before I reached the 5 mg dose, the point where it kicked in for me, the hunger had my full attention. I would sit at work counting the hours until I was allowed to eat again, a low-key negotiation running underneath everything else I was supposed to be doing. Then the dose climbed and that just went quiet. I could hear myself think and eat normally without the everpresent noise. That is the part the medication does, and it is not small. For me the appetite was the whole problem, and nothing else I tried mattered until it got solved.
But the drug does not lift anything. It does not weigh your chicken. It does not show up at 6 a.m. in the gym. The body underneath the fat got built by the boring stuff around the prescription.
I climbed the dose slowly, which surprises people who assume you rush to the maximum dose as quickly as possible. I never even made it to the 15 mg top dose. I was not in a hurry, and the appetite control on the middle doses was plenty for me.
Underneath it, the unglamorous machinery. I tracked all my food in MacroFactor, which sets a calorie target and adjusts it based on what the scale actually does instead of a formula. My protein started embarrassingly low, around 100 grams a day, and ramped to about 200 once I knew it mattered. Six months in (May 2025) I hired a coach through the Future Pro app and started lifting four to five times a week. Testosterone replacement played a role too, which I have written about and will not re-litigate here.
What I did not do is eat clean in any influencer sense. I eat a lot of fruit. Healthy Choice Cafe Steamers became my staple, a frozen meal in the microwave in four minutes with the calories printed on the box. I go through think! White Chocolate protein bars at a rate I am not proud of. The whole thing was convenient, partly processed, calorie-controlled, and tracked. If you are waiting until you can cook like a chef to start, you will wait forever. I lost 170 pounds on frozen meals and protein bars, not a special diet.
On the macros, I kept protein high on purpose and did the rest by feel. I ran fat fairly low, partly because I am a kid of the 80s when fat was the enemy, and partly because I really like fruit, which kept my carbs higher than the low-carb crowd would ever sign off on. It did not seem to matter. The protein and the calorie deficit did the work.
Why I lost more than the trials predict
My numbers are not typical, and I want to be straight about why. In SURMOUNT-1, the big tirzepatide trial, people lost about 21 percent of their body weight at the top dose over 72 weeks. I lost about 45 percent, and I never went past 12.5 milligrams. That puts me in what people call hyper-responder territory, which is not an official medical category, just a way of saying the drug happened to work unusually well on my particular biology. Researchers are starting to map the genetics of who responds to these drugs and who barely responds at all.
The clinical scorecard makes the same point from the other side. In the tirzepatide trials, the two strongest predictors of a big weight response are being female and being younger. Women were about two and a half times more likely than men to lose 15 percent or more, and the odds slip with every five years of age. I am a 53-year-old man. What I had going for me was a normal HbA1c, because I was never diabetic, and a fast early response, but that doesn’t explain losing more than twice the average. By the numbers a doctor can actually measure, I was a middling bet who landed at the far end of the curve.
I got lucky there, and I did not earn it. What I did earn is everything I bolted onto that luck: the slow titration, the tracking, the protein, the lifting, the testosterone that holds onto muscle while you lose fat. None of it is exotic. The response itself was luck. Everything I did with it, I earned.
Gaining muscle in a calorie deficit
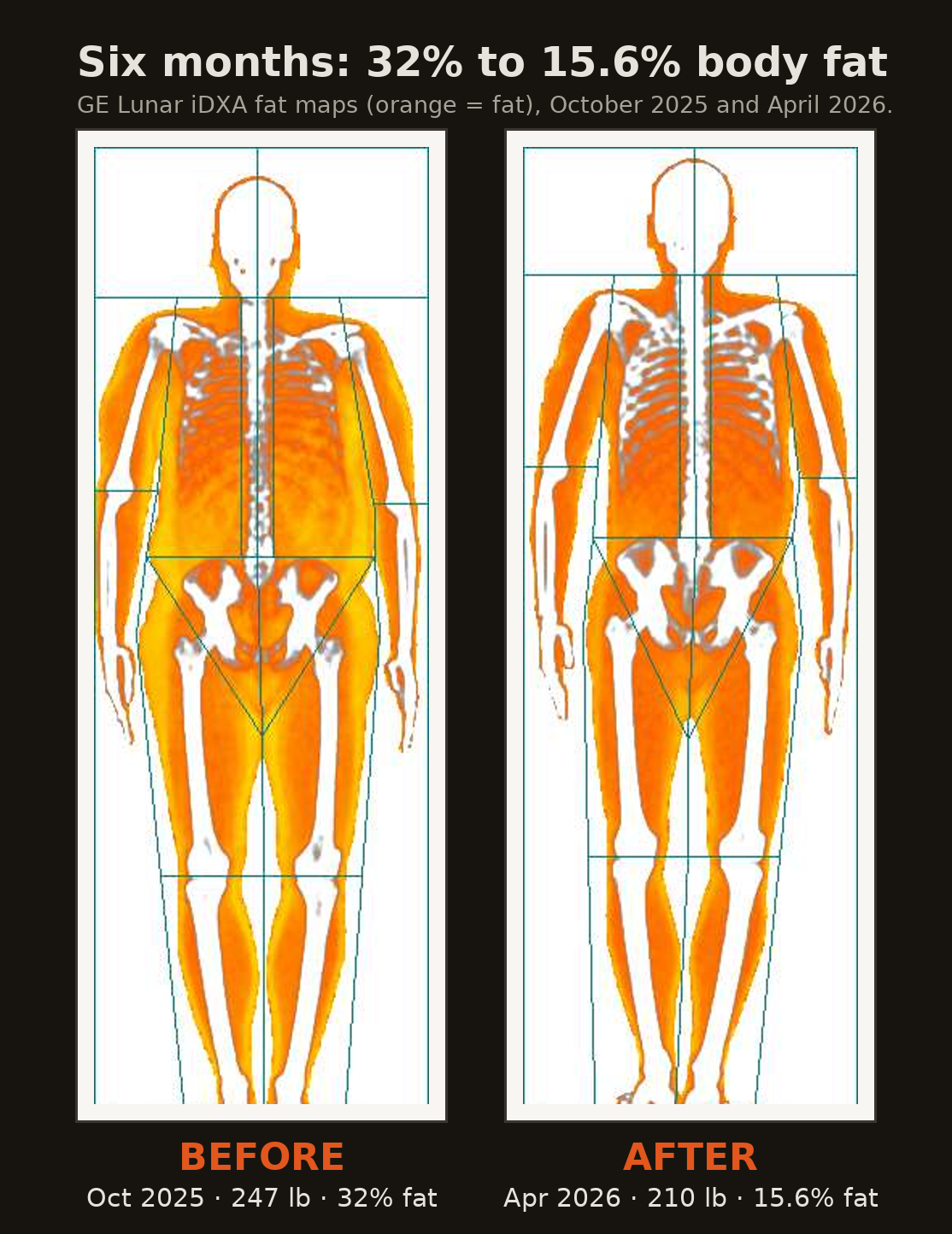
During the journey I got two DEXA scans, six months apart near the end of the journey. In October 2025 I was 247 pounds at 32% body fat, with 161.6 pounds of lean mass. By April 2026 I was 209.5 pounds at 15.6% fat, with 171.2 pounds of lean mass. Read that again, because I had to. I lost 44 pounds of fat and gained almost 10 pounds of muscle in the same six months, while eating in a deficit. DEXA is not divine truth, but the change was too large to dismiss as water and glycogen. The visceral fat, the dangerous kind packed around the organs, was cut in half, from 147 to 66 square centimeters. Most references put the line for elevated metabolic risk somewhere around 100, so I went from well over it to comfortably under.
Gaining muscle while losing fat is supposed to be hard, and I want to be honest about why it was possible for me. I was very heavy and very out of shape, and I was on testosterone. That is body recomposition on the easiest setting the universe offers. My body had enormous fat reserves to fuel the work, my muscles had decades of catching up to do, and the hormones were finally in the right place. Newbie gains on TRT made it possible.
So calibrate this against yourself. If you are a lean 45-year-old who has trained hard for fifteen years, you are not going to lose 44 pounds of fat and add 10 of muscle in six months. The further you are from your potential, the more dramatic the change looks. I was about as far from mine as a person can get, and that is exactly why the recomposition was so steep.
My metabolism was supposed to crash. It didn’t.
This was what genuinely worried me going in. The story everyone knows about big weight loss is that your metabolism collapses and drags you back. The Biggest Loser contestants are the cautionary tale: years after the show, many were burning hundreds of calories a day less than their body size predicted, fighting their own physiology to keep the weight off. The body defends its old set point.
In April I paid for a metabolic test, the kind where you breathe into a mask while chilling in a recliner to measure what you actually burn at rest. My resting metabolic rate came back at 2,157 calories, which is about 10% higher than the standard equations predict for someone my size. Not lower. Higher. The thing that is supposed to happen did not happen.
The likely reason is muscle, though I would not pin the whole 10 percent on one cause. The lean tissue I kept and built is metabolically expensive, and there was a lot of it for my weight. Lifting kept building it instead of letting it waste away the way it does on a crash diet, and the testosterone certainly helped. In practice it means I now eat around 2,800 calories a day and hold steady. I did not just lose the weight, I built a body that is set up to hold it. That is a better starting point for maintenance, not a guarantee I will never regain.
The cardio test I was too scared to take
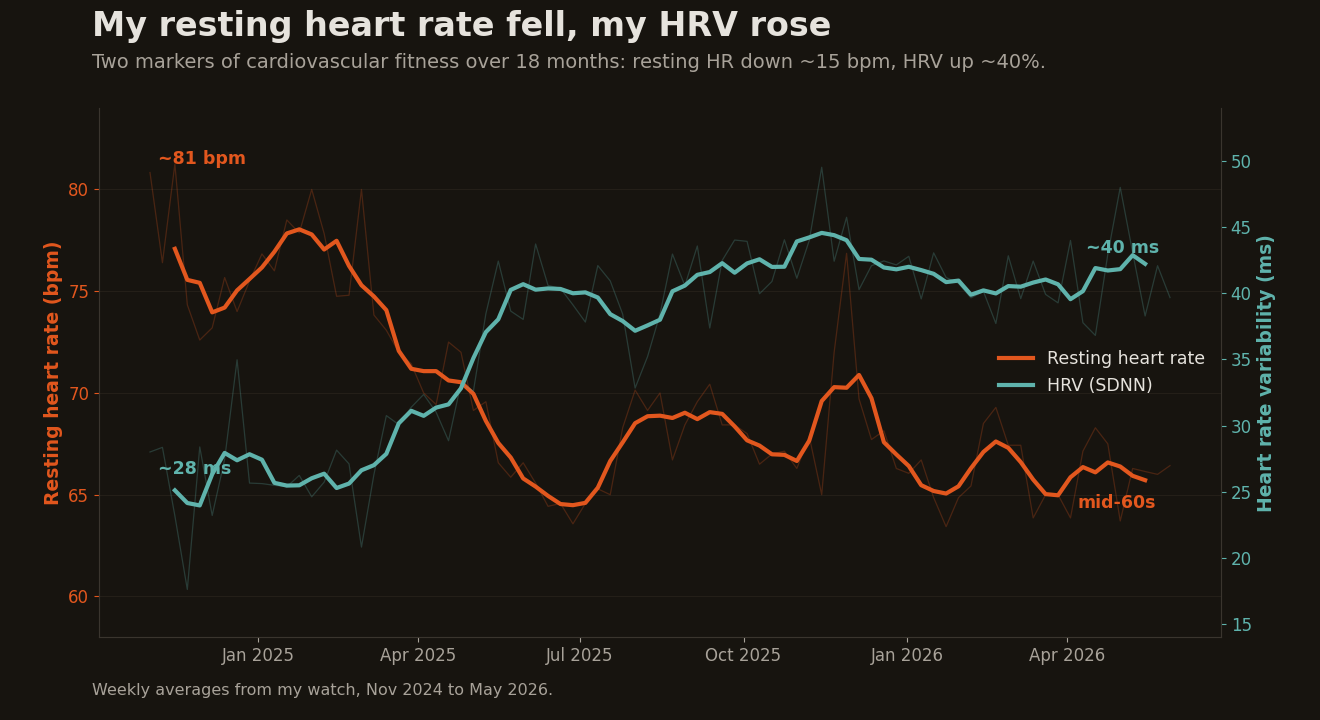
I never measured my cardio fitness at the start, the same way I never got that baseline DEXA. But two numbers my watch tracked the whole way tell the story anyway. My resting heart rate fell from the low 80s to the mid-60s, a drop of about 15 beats a minute. My heart rate variability, a rough readout of how recovered and resilient your nervous system is, climbed from the high 20s into the low 40s. Neither is a perfect metric, but both moved the right direction, steadily, over eighteen months. A heart that beats fifteen fewer times a minute at rest is doing less work all day, which matters more to me than to most people, for a reason I will get to.
What I wanted was a real VO2 max, the gold standard for aerobic fitness. I do not have one because I have been too intimidated to book the lab test, the one where they strap a mask on you and run you to exhaustion. So I did the version I could face. In January I rowed a hard 5K on the Concept2 in my garage and finished in 19 minutes and 29 seconds, averaging about 219 watts, with my heart rate pinned in the top zones the whole way. That was faster than I expected.
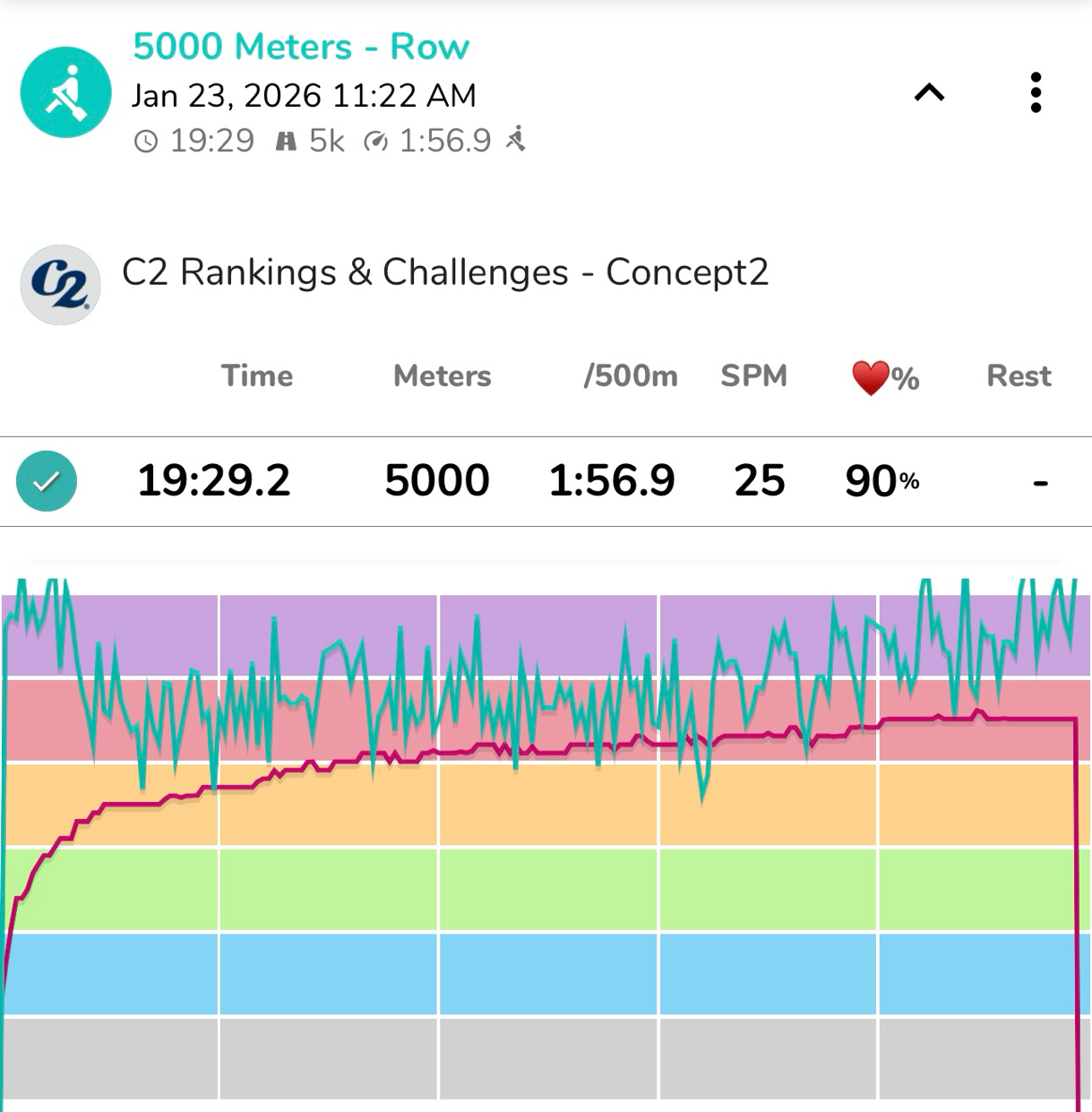
Translated into VO2 max, that effort works out to around 40, give or take a few points, which apparently is good-to-excellent for a 53-year-old man, and better than it sounds once you remember I was still hauling 216 pounds across the rower. The rowing calculators online will hand you a rosier number, but the oxygen math behind 220 watts does not quite support it. It is an estimate, not a lab number. But it is a real benchmark I can run again in the same garage, which beats a number I am too nervous to go get.
LDL hit 131, then 60
Not everything moved in a straight line. In January 2025, a few months in and dropping weight fast, my LDL cholesterol jumped to 131. That felt backwards. I was doing everything right and the number got worse. It turns out this is a known and temporary thing. When fat cells shrink quickly they dump their stored lipids into the bloodstream, and your cholesterol can rise during rapid loss even as the underlying picture improves. It came back down as the loss continued. If you see this on your own labs mid-journey, do not panic and do not quit.
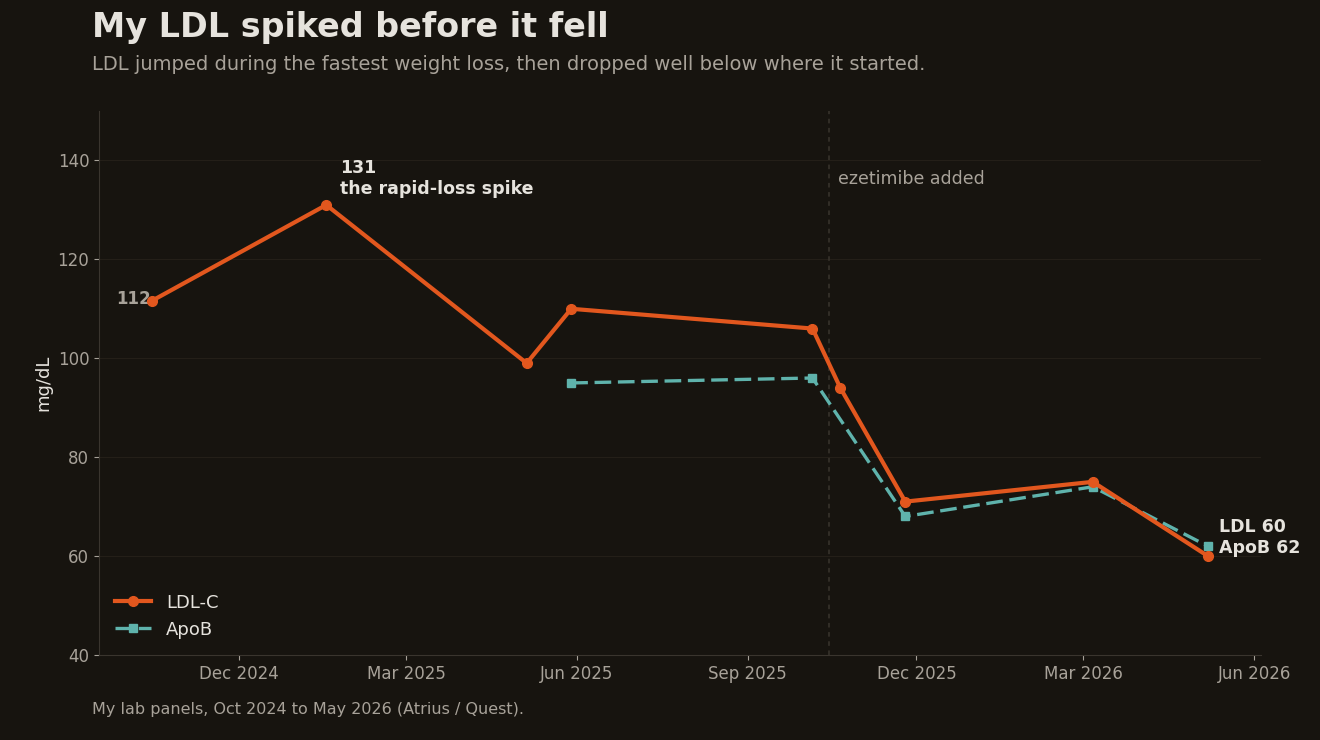
Where those numbers sit now is what I am proud of. My LDL is 60 and my ApoB, the better marker, is 62, helped by adding ezetimibe in October 2025. My triglycerides went from 227 to 63. My hs-CRP, a measure of systemic inflammation, dropped from 2.83 to under 0.2, which is about as low as that test reads. Some of that is the weight coming off. The trials also show tirzepatide lowering inflammatory markers like CRP and IL-6, some of it independent of weight loss, though in my own case I cannot cleanly separate the drug from everything else that changed.
I care about these numbers more than most people my age have to, for a specific reason. A routine calcium score test in February 2026 found an aneurysm in my ascending aorta, measured at 4.64 centimeters. It’s well below the threshold to merit surgical intervention but high enough to get the scary “aneurysm” label. That reframes everything. For me, an optimal LDL and well-controlled blood pressure are not health optimization, they are critical management of a weak spot in the most important pipe in my body. I take telmisartan, which lowers blood pressure and eases stress on the aortic wall at the same time. It is also the quiet reason I chose tirzepatide over exploring the newer, more potent drugs that push heart rate higher. When you have a number on your cholesterol panel that actually means something, you stop treating it like a vanity metric.
I stay on the full dose on purpose
I am still taking 12.5 mg every week, and I plan to keep taking it. People (including initially my PCP) assume the arc is that you take the drug, lose the weight, and lower the dose or get off it. I had assumed I would go back to 10 or even 5 mg, the lowest maintenance dose, until I looked at what actually happens when people stop.
The question I had was narrower, whether you could hold the loss on a lower dose, and for a long time nobody had run that trial. I wrote a whole post wishing for that exact trial. This spring it finally ran. SURMOUNT-MAINTAIN took people who had lost a lot of weight on the full dose and split them three ways for a year: stay on the full dose, drop to 5 mg, or switch to placebo. The full dose held the loss best, about 22 percent below starting weight. The 5 mg group kept most of it, about 17 percent down. The placebo group gave a real chunk back, to about 10 percent. One more way to see it: 8 percent of the full-dose group regained more than half of what they had lost. On 5 mg it was 25 percent. On placebo, 67.
That is not a surprise once you accept what the drug is doing. It is managing an appetite that, left alone, put 170 pounds on me. Take the management away, even partway, and some of it comes back. The 5 mg result is genuinely useful, because it says I could probably hold most of my loss on a lower dose if I needed to. But “most” is carrying a lot of weight in that sentence, and the full dose is the arm that worked best. So for now I stay where I am. That is my call, made with my doctor, my labs, and my reasons. Yours might land somewhere else.
So I treat this the way I would treat any chronic condition. I stay on the medication, I eat at maintenance, around 2,800 calories and 200 grams of protein, I lift five times a week, and I hold somewhere between 200 and 210 pounds. One morning the scale read 199.3 and I took a photo, because getting under 200 is its own small milestone. I am not immune to thinking about those. But my real number is the low 200s, and I am not chasing the photo. I am holding the line, on purpose, with a plan.
Get the free Bloodwork Decoder
You saw what my own labs did over the rebuild. I turned everything I learned reading my panels into a one-page cheat sheet: what every number means, what to aim for at 50, and what to ask your doctor. Subscribe free and I’ll send it to your inbox. No spam, nothing to sell.
What I’d tell the guy in 2021
There is a version of me from a few years ago mid pandemic lockdown, sitting in the guest room at well over 350 pounds, doing the kind of math where you quietly wonder how many good years are actually left. If I could tell him one thing, it would not be “you can do it.” It would be that the thing that finally worked was not just willpower. It was a tool that solved the appetite and a plain system built on top of it: track the food, eat the protein, lift the weights, check the labs, and keep going on the days nothing feels different.
None of it is free. It is a prescription I plan to keep, lab draws every few months, and a routine I do not get to quit.
But I fit in the airplane seat. I can shop in the regular section. My bloodwork looks like a different person’s, and the metabolic test says the body I rebuilt is set up to keep it that way. At 53, after most of my adult life going the other direction, that is the rebuild. It is not finished, because it does not get to be finished. It just gets to be maintained.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.