

The question I have been asking
Get the next one in your inbox
I cover the latest GLP-1 trials and access changes weekly. Free, no spam, unsubscribe whenever.
I am eighteen months into Zepbound and at the body weight I actually want to hold. Two hundred and five pounds, down from three hundred and seventy three. The DEXA scan I had in April said I had lost a hundred and seventy pounds of fat and gained nine and a half pounds of lean mass in the process. The TRT article I published yesterday walks through how all of this came together. This post is about what comes next.
The question when you are at goal is one I have been turning over for months. You can keep injecting at the dose that got you here. You can drop to a lower maintenance dose. You can come off the shot entirely and hope a daily pill, when one is approved for maintenance, is enough. Or you can stop, and accept the likely weight regain.
Three days ago I told r/ProactiveHealth that ATTAIN-MAINTAIN was not the trial I actually wanted. ATTAIN-MAINTAIN, published in Nature Medicine on May 13, takes patients off the injectable tirzepatide entirely and switches them to a daily oral GLP-1 pill called orforglipron, or to placebo, for a year. People who switched to the pill kept about three quarters of their weight loss. That is a real and useful answer, especially for the access and cost side of GLP-1 maintenance. It just does not answer the question I have, which is the more simple one: if I stay on the injection but drop the dose, do I hold the line.
That trial finally landed this week. It is called SURMOUNT-MAINTAIN and it was published in The Lancet on May 12. It is Lilly-funded. It randomized three hundred and seventy-eight adults with obesity at exactly the point I am at right now, body weight plateaued after a long open-label run of tirzepatide, into three roads.
What SURMOUNT-MAINTAIN actually tested
The design is cleaner than most trials in this space. Everyone in the trial spent sixty weeks on open-label tirzepatide at the maximum dose they could tolerate, either ten or fifteen milligrams a week (I am on 12.5mg and 75 weeks in). Sixty weeks is long enough that body weight had time to plateau, and eighty four percent of participants did plateau by the time the second phase started. At that point the trial randomized them into three groups for the next fifty-two weeks of double-blind treatment.
The first group continued tirzepatide at the same maximum tolerated dose they had been on. The second group dropped to five milligrams a week. The third group switched to placebo. Everyone kept getting lifestyle counseling from a dietitian and was allowed to use rescue tirzepatide if they regained more than half of what they had lost. That rescue rule is unusual and worth keeping in mind, because it means the placebo arm result is the regain you would see in someone who has access to ongoing care, not the unsupported worst case.
Baseline numbers say something about who was in this trial. The median age was forty-seven. Sixty-five percent of participants were women, thirty-five percent were men. The starting BMI was forty, falling to thirty-one by the time of randomization. People had been living with obesity for a median of thirteen years before they entered the trial. This is not a vanity trial. These are people with serious cardiometabolic risk who finally got something to work (I went from a BMI of 41 to 25).
The numbers
The primary endpoint was percent change in body weight from the original baseline at week one hundred and twelve, which is the end of the maintenance period. The three arms separated cleanly.
People who stayed on tirzepatide at the maximum tolerated dose ended the trial at twenty-two percent below their starting weight. People who dropped to five milligrams ended at seventeen percent below. People who switched to placebo ended at ten percent below. The p-values are all less than 0.0001, which at this sample size is just shorthand for the result being real.
The more useful framing for someone in my position is the change from the randomization point, not from baseline, because that measures what each arm gave back during the maintenance phase. The maximum-dose group gave back essentially nothing, two-tenths of a percent. The five-milligram group gave back seven percent of body weight, about thirteen pounds. The placebo group gave back fifteen percent, about twenty-eight pounds, and most of them needed rescue medication along the way.
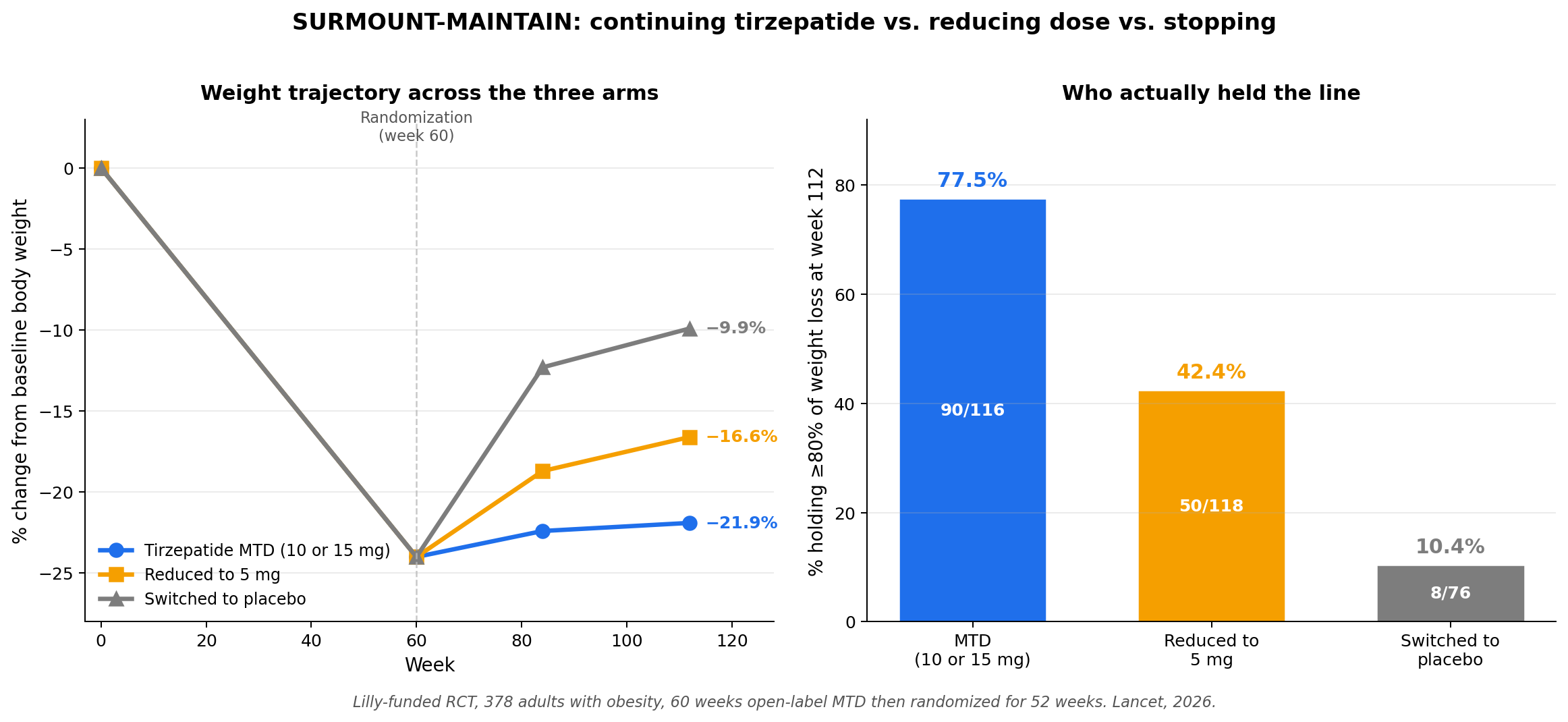
The cleanest single metric, in my view, is the one on the right side of that chart. Among people who had reached a body weight plateau during the open-label phase, what fraction held onto at least eighty percent of their initial weight loss after fifty-two weeks in the maintenance phase. Holding onto eighty percent of a loss is a reasonable practical definition of “this worked.” Seventy-eight percent of the maximum-dose group cleared that bar. Forty-two percent of the five-milligram group cleared it. Ten percent of the placebo group cleared it.
Translated into the language of odds rather than percentages, compared to switching to placebo, staying on the maximum dose made you about seven times more likely to hold the line and dropping to five milligrams made you about four times more likely. The maximum dose is plainly better. Five milligrams is plainly better than nothing. The space between five milligrams and the maximum dose is the live clinical question.
Two more numbers from the trial that get less attention but matter. First, the proportion of participants who needed rescue tirzepatide during the maintenance phase. Eight percent of the maximum-dose group, twenty-five percent of the five-milligram group, and sixty-seven percent of the placebo group. Two-thirds of the placebo arm needed rescue. This is the most direct evidence I have seen that going to zero on an obesity medication after substantial weight loss is not, for most people, a viable plan.
Second, the gastrointestinal side effects. Fourteen percent of the maximum-dose group had nausea, vomiting, or diarrhea during the maintenance phase. Seven percent of the five-milligram group did. Three percent of the placebo group did. The dose-response is real. If the maximum dose is wearing you down with GI side effects after a year, dropping to five milligrams is a tolerability win that costs you a meaningful but not catastrophic amount of efficacy.
What this means if you are at your goal weight
I have spent the last week running these numbers against my own situation. The framework I have landed on is straightforward.
If you are at your goal weight on tirzepatide and tolerating the dose well, the trial says staying at the maximum tolerated dose is your best shot at holding the line. Ninety-seven percent of the weight loss preserved on average. Seventy-eight percent chance of being what the paper calls a “maintainer.” Two-thirds lower rescue rate than the five-milligram group. The cost is whatever GI side effects and injection burden you are already living with, plus whatever the medication is costing you per month, plus whatever you would otherwise have done with the metabolic capacity to eat more.
If the maximum dose is genuinely difficult to tolerate, dropping to five milligrams is a real option. You give back roughly six kilograms over a year, plus or minus, and your odds of being a “maintainer” fall by about a third. Some of that giveback is probably water and lean tissue rather than fat, but the trial did not characterize this and I will come back to that gap. The trade is a meaningful loss of efficacy in exchange for fewer side effects, lower monthly cost in the US given the current dose-by-dose pricing structure, and a more sustainable life trajectory.
If you are thinking about stopping the medication entirely and want to know what the trial actually shows about that road, the honest answer is that the trial shows it does not work for most people, even with continued lifestyle counseling. About ninety percent of people who stopped did not hold onto most of their weight loss. The rescue-medication uptake in the placebo arm tells you the same thing in different language. The narrative that some people coast off these drugs and keep the weight off through grit and discipline alone, and that this is the goal you should be aiming at, is contradicted by every randomized trial that has actually tested it.
The trial does not, on its own, tell you what to do. It tells you what to expect from each of three roads. The decision is yours, your doctor’s, and your insurer’s. For my own answer, I am staying at the maximum tolerated dose for now. The reason is not that I cannot live with thirteen pounds of giveback. It is that the trial shows the dose I am on right now is doing the thing I am paying it to do. The maintenance dose, the data suggest, is the dose that actually maintains. I will just adjust my calorie targets to eat at maintenance or even slight surplus to build muscle. If eating enough is too hard, I might drop down a notch to 10mg.
What the trial did not answer
The most important gap in SURMOUNT-MAINTAIN is body composition. The trial did not measure fat-versus-lean composition of the weight gained back in the five-milligram group or the placebo group. That matters. Weight regain that is mostly fat is one kind of giveback. Weight regain that includes lean mass and bone density is another, especially for people my age. The paper itself flags this and says it warrants further study. I would like to see the DEXA data.
The trial ran fifty-two weeks of maintenance. That is one year. Tirzepatide is now being used for what will, for most people on it, be a multi-decade course of therapy. SURMOUNT-MAINTAIN tells you what happens over the first year of maintenance. It does not tell you what happens at year three or year five. The five-milligram weight curve in particular did not appear to plateau at week one hundred and twelve, which raises the question of whether the giveback continues to accumulate over time, or whether it stabilizes. We will not know until the longer follow-up data lands.
The trial excluded people with diabetes at baseline. This is reasonable for trial design but means the results apply most cleanly to people, like me, who are using tirzepatide for obesity without a diabetes diagnosis. Whether the dose-reduction strategy translates as cleanly for someone using the drug for both type 2 diabetes and weight management is a different question.
The trial also did not break out results by sex. Thirty-five percent of participants were men. That is enough men to power some kind of subgroup analysis, but the published paper does not give one. Whether male-specific factors like baseline lean mass, testosterone status, or visceral fat distribution change the dose-reduction calculus is the kind of thing I would love to find in the supplement, and I will dig through the appendices and update this post if anything substantive comes back.
Finally, the trial is Lilly-funded and ran in Lilly-friendly academic centers. Definitely interesting. Definitely not the last word.
What I am doing about it
I am staying at the maximum tolerated dose. Marek Health monitors my labs every few months and they have not flagged anything that would suggest the dose is becoming a problem. I am not suffering GI side effects. My DEXA composition is moving in the direction I want it to. I will revisit this decision when SURMOUNT-MAINTAIN’s longer follow-up lands, when a body composition substudy publishes, or when my own bloodwork or quality-of-life experience changes the math. For now the trial confirms what I had been guessing, which is that the dose that gets you to goal is also, more or less, the dose that holds you there.
If you are in the same position and your doctor has been talking about dose reduction (like mine has!), the conversation is now better-informed than it was a week ago. You can decide with real numbers rather than vibes. That, more than anything else, is what SURMOUNT-MAINTAIN actually delivered.
I keep a running tracker of every GLP-1 and incretin drug, approved and still in the pipeline, with what each one targets, how far along it is, and what's coming next.
See the full GLP-1 Pipeline Tracker →About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.