

I’m 53 years old and 170 pounds lighter than I was a year and a half ago. That’s the number everyone asks about. It’s also the wrong number.
The number that actually tells the story is one the bathroom scale never showed me. Over one six-month stretch, the scale said I’d lost 35 pounds. The DEXA scan said something very different: I’d dropped 44 pounds of fat and added 9 pounds of muscle. The scale had quietly averaged those two things into one misleading figure. What was really happening was body recomposition, and at 53, on a GLP-1, after decades of being heavy and out of shape, almost everyone would have told me it was off the table.
It wasn’t. It was the predictable result of doing specific things while the fat came off. This is the post I wish someone had handed me when I started, because the recomposition is the part that matters and it’s the part nobody puts on the scale.
The number the scale was hiding
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
Here are the actual readouts, because the gap between them is the whole point.
I had two DEXA scans six months apart, October 2025 and April 2026. A DEXA is the body-composition scan that splits you into fat, lean mass, and bone instead of mashing it all into one weight. Between those two scans my total fat mass went from 76 pounds to 32. My lean mass went from 162 to 171. My visceral fat, the dangerous stuff packed around the organs, fell from a VAT area of 147 square centimeters to 66. My android-to-gynoid ratio, basically how much of my fat sat around the belly versus the hips, dropped from 1.39 to 0.96. I finished at 15.6 percent body fat, which I hadn’t seen since my twenties.
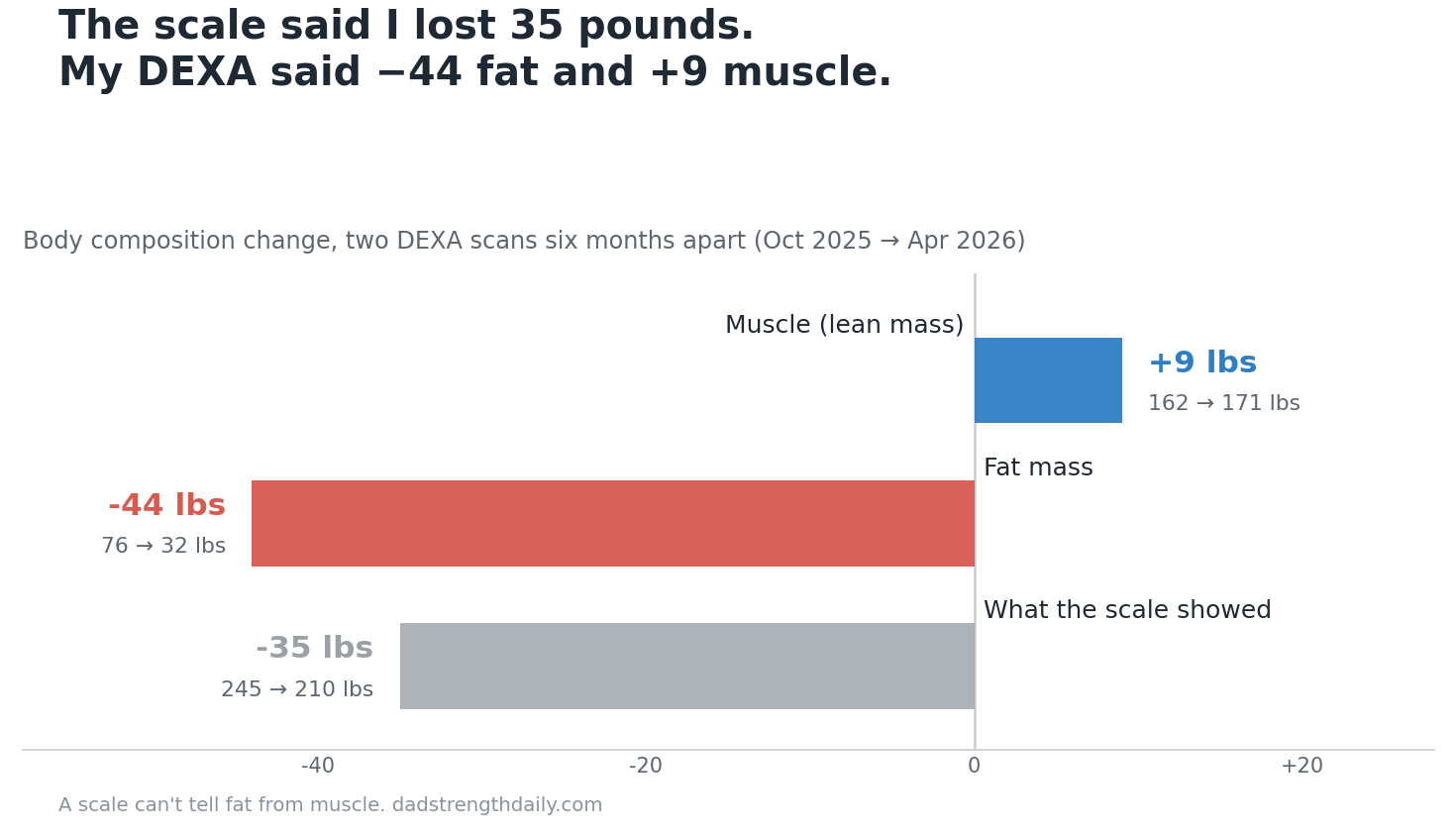
Now put that next to the scale. The scale moved 35 pounds over those six months. If I’d trusted it, I’d have assumed I lost 35 pounds of “weight,” some mix of who knows what, and moved on. Instead I lost 44 pounds of pure fat and built 9 pounds of muscle underneath it. The scale took my biggest win, the 9 pounds of new muscle, and subtracted it from the fat loss to hand me one flattened number. It hid the muscle by design.
This is why I get a little evangelical about it. If you’re doing this right, the scale will undersell you. It’ll move slower than you think it should, and some weeks it won’t move at all, while underneath you’re trading fat for muscle pound for pound. A scale can’t tell the difference between a pound of fat and a pound of muscle. Your body can, and so can a DEXA.
What recomposition actually is
Recomposition, “recomp” if you spend any time in the lifting corners of the internet, is losing fat and gaining or at least holding muscle at the same time. That’s it. It sounds modest until you notice the entire fitness industry is built on the assumption that you can’t do both at once, that you have to pick a “bulk” or a “cut” and alternate between them like you’re running a tiny factory.
For a lot of people that assumption holds. For a specific and very large group it’s wrong, and that group includes most men over 50 who are carrying extra weight and haven’t trained seriously in years. I was the poster child. At 373 pounds I wasn’t short on reserves. My body had enormous stores of fat it could pull from to build and repair muscle while I ate at a deficit. That’s the quiet engine under recomposition: when conditions are right, your body will fuel muscle growth out of your fat stores instead of out of your plate.
Your body is constantly deciding where calories and amino acids go, and that process has a name, nutrient partitioning, but you don’t need to memorize it. The practical version is what matters: muscle is metabolically expensive, so your body only keeps and builds it when something is loudly telling it to. That something is resistance training plus enough protein. Take those away and a body in a calorie deficit does the thrifty thing. It burns some fat and dismantles some muscle, because why hold onto an expensive tissue nobody’s using. That’s the default setting. Recomposition is what you get when you override it.
Who actually gets to recomp (the honest version)
I’m not going to sell you the idea that everyone gets my result, because that’s exactly the overpromising that makes most fitness content useless. Recomposition is real, but it’s far easier for some people than others, and being honest about who’s in the easy group is the difference between advice and a pitch.
The people who have it easiest are the ones new to training, or coming back after a long layoff. Untrained muscle responds fast, the so-called newbie gains, and “newbie” at 53 absolutely counts even if you lifted in college. It’s also easier if you’re carrying a lot of fat, because you’ve got the fuel on board to build muscle without eating in a surplus. And hormones tilt it. For me that meant testosterone replacement, which I’ve written about separately, and which genuinely helps the body hold and build muscle at my age.
I had all three going for me. I was deeply detrained, I was very heavy, and I was on TRT. That’s recomposition on easy mode, and I want to name it plainly so you can calibrate against your own situation. If you’re a lean 45-year-old who has trained hard for fifteen years, you’re not going to lose 44 pounds of fat and add 9 of muscle in six months, because you don’t have 44 pounds of fat to give and your muscle is already near its natural ceiling. For you, recomp looks like slowly leaning out while holding your strength, which is still a win, just a quieter one. The further you are from your potential, the more dramatic the change. The closer you are, the more it becomes a maintenance job. If you’re overweight and out of practice the way I was, your body is primed to do both at once, and most people waste that window.
The GLP-1 catch: the drug doesn’t protect your muscle
Here’s where I have to be careful, because I take a GLP-1 and I’m not going to pretend it did nothing. Tirzepatide did the single hardest thing in all of weight loss. It quieted my appetite so that eating at a deficit stopped feeling like a daily fight with myself. If you want the full story of the drug and the dose, that’s a different post.
But the drug did not protect my muscle, and this is the part the glossy coverage skips. Left alone, a GLP-1 will let you shed muscle right alongside the fat. Depending on the study, somewhere between a quarter and 40 percent of the weight people lose on these drugs can be lean mass if they do nothing about it. That’s an enormous amount of muscle to hand over, and after 50 you don’t make it back easily. The appetite suppression that makes the fat loss so easy is the same thing that makes muscle loss so likely, because when you barely feel like eating, the first casualty is usually protein.
It gets more pointed in the maintenance phase. A lot of people now ride these drugs down to a lower dose or space the shots out once they’ve hit their goal, which is a reasonable thing to do and something I dug into when I wrote about the SURMOUNT-MAINTAIN trial. But maintenance is exactly when people relax the protein and quit the gym, and that’s when the muscle you protected on the way down can quietly slip away. The drug’s job ends at appetite. Everything about your body composition, the part that decides whether you end up lean and strong or just smaller and soft, is on you.
The two levers: protein and the barbell
I protected my muscle with two things, and honestly the rest is rounding error.
Protein came first, always. I aimed for roughly one gram per pound of my target body weight, which put me around 200 grams a day, and I hit it often enough that it counted. That’s a lot of protein when a drug has switched off your hunger, and it took real intent: protein on the plate before anything else, Greek yogurt and poultry and beef doing most of the work, a shake when whole food wasn’t realistic. I tracked it in an app so I wasn’t kidding myself, because “I eat pretty high protein” is almost always a lie when you actually count. Protein is the raw material muscle is built from, and in a deficit it pulls double duty by signaling the body to hold what it has. I went deeper on the specific numbers in my post on protein for keeping muscle on a GLP-1, and if you take one practical thing from this entire piece, make it the protein target.
The other lever is resistance training, and it’s the one that does the talking. Lifting is the signal that tells your body these muscles are in use, don’t break them down for parts. I lifted the whole way down, and I kept lifting, mixing the barbell with indoor cycling and rowing for the heart. You don’t have to live in the gym to send that signal. Two or three honest strength sessions a week will carry most of the load, as long as they’re actually hard and you’re trying to add weight or reps over time. That last part, progressive overload, is the thing beginners skip. Doing the same comfortable weights forever tells your body nothing. Picking up something a little heavier than last month tells it everything.
For a 50-something specifically, a few things matter more than they did at 25. Compound movements give you the most muscle for your time, some version of a squat, a hinge, a push, and a pull, and machines are completely fine if your joints prefer them. Recovery is slower now, so two quality sessions beat five rushed ones. And you have to actually approach failure on your hard sets, because the polite three-sets-of-ten you can do while holding a conversation isn’t a strong enough signal. I’ve laid out the over-50 version of all this in how to build muscle after 50, and the flip side, what actually drives the muscle loss in your 50s, is worth reading if you want the mechanism.
The cardio I did for my heart and my conditioning, not because it drives recomposition. I’d gently steer you away from thinking you can run or row your way to a recomp. The lifting is the lever that moves body composition. The cardio is so you’re around to enjoy the muscle, and it earns its place on those terms.
Everything people obsess over past those two levers, the supplements, the meal timing, the fasted-versus-fed cardio debates, is small change next to protein and progressive resistance training. The evidence-minded training people I actually trust, the ones who read the studies instead of selling the powder, land in the same spot every time. Get your protein, lift with intent, be patient.
Where people blow it
I watched a lot of people in the GLP-1 world get the weight loss and waste the recomposition, and it’s almost always the same handful of mistakes.
The biggest one is letting protein collapse because the appetite is gone. The drug makes it genuinely hard to eat, so the path of least resistance is a few hundred calories of whatever’s easy, and muscle pays for it. The second is doing all cardio and no lifting, usually because cardio is easier to start and the scale rewards it early. The scale loves muscle loss, remember, because muscle is heavy. The third is crashing the deficit too hard, slamming calories so low that the body can’t build anything and starts breaking down muscle for fuel even with protein and training in place. And the last one is the saddest, quitting the lifting the moment the weight is off, right when holding the muscle becomes the entire game.
None of these are willpower failures. They’re just what happens by default when a drug removes the hunger that used to organize your eating. You have to put a new structure in its place on purpose.
Why I trust the DEXA over the scale and the mirror
If recomposition is invisible on the scale, you need a better instrument, because the scale and the mirror lie to you in opposite directions. The scale tells you nothing’s happening, because new muscle is masking the fat loss. The mirror flatters or crushes you depending on the light and your mood. Neither gives you a number you can steer by.
A DEXA does. For somewhere around a hundred dollars at most city imaging centers, you get fat, muscle, and visceral fat broken out, plus a baseline to measure against six months later. The visceral fat number alone is worth the trip, because that’s the fat driving the metabolic and cardiovascular risk, and you can’t see it or feel it. Mine fell by more than half between scans and I’d never have known from the outside. The scan also reads your bone density, which matters more than people expect during fast weight loss, since dropping weight quickly can cost bone along with fat, and resistance training is one of the few things that protects it. I wrote up the whole experience of getting a DEXA during GLP-1 weight loss, including what to ask for and how to read the report, because the report is genuinely confusing the first time you see it.
Get a baseline before you start, or early, if you can. If you’ve already started, get one now, because a scan today plus a scan in six months still tells you the one thing that counts, which direction your body composition is actually moving. Watch the lean mass and the visceral fat, not just the number at the bottom. And give it time. Recomposition is slow by nature, because building muscle is slow even under ideal conditions, and the whole thing only shows itself over months.
A few honest caveats, since I’ve been honest this far. I had unusual advantages: the TRT, a very high starting weight, a strong response to the medication. Your numbers will be your own. Talk to a doctor before you start a GLP-1 or change your training if you’ve got medical history that matters, and don’t read my DEXA results as a forecast of yours.
But the principle under those numbers isn’t unusual, and it doesn’t require a drug or a hormone or a lucky gene. Protect muscle with protein and resistance training while the fat comes off, and your body will trade one for the other, and the scale will badly understate what you did. I lost 170 pounds. The only reason I know that most of what I kept was muscle and most of what I lost was fat is that I stopped trusting the scale and started measuring the thing that actually counts.
I keep a running tracker of every GLP-1 and incretin drug, approved and still in the pipeline, with what each one targets, how far along it is, and what's coming next.
See the full GLP-1 Pipeline Tracker →About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.