

I’m 170 pounds down on tirzepatide, 18 months in. Somewhere around the 80-pound mark, the questions from people I hadn’t seen in a while shifted. It used to be “what are you doing?” Now it’s “is it keto?” Always keto. Not once “is it Mediterranean?” Not once “did you cut sugar?” Not even “is it Ozempic?” Just keto.
It reminded me of the late 2010s, when everyone who heard any electronic music for the first time asked “is this dubstep?” It usually wasn’t dubstep. But dubstep was the one word they had. Keto has become the dubstep of weight loss: a single term doing the work of a whole genre most people cannot tell apart.
I was not doing keto. I was counting calories, limiting sodium and taking tirzepatide, plus more protein, plus training. But I get why people ask, because the diet world has scrambled these words into mush and somehow keto became the most successful one. Here is what they actually mean.
The carb-restriction family
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
Three terms get used almost interchangeably, and they should not be.
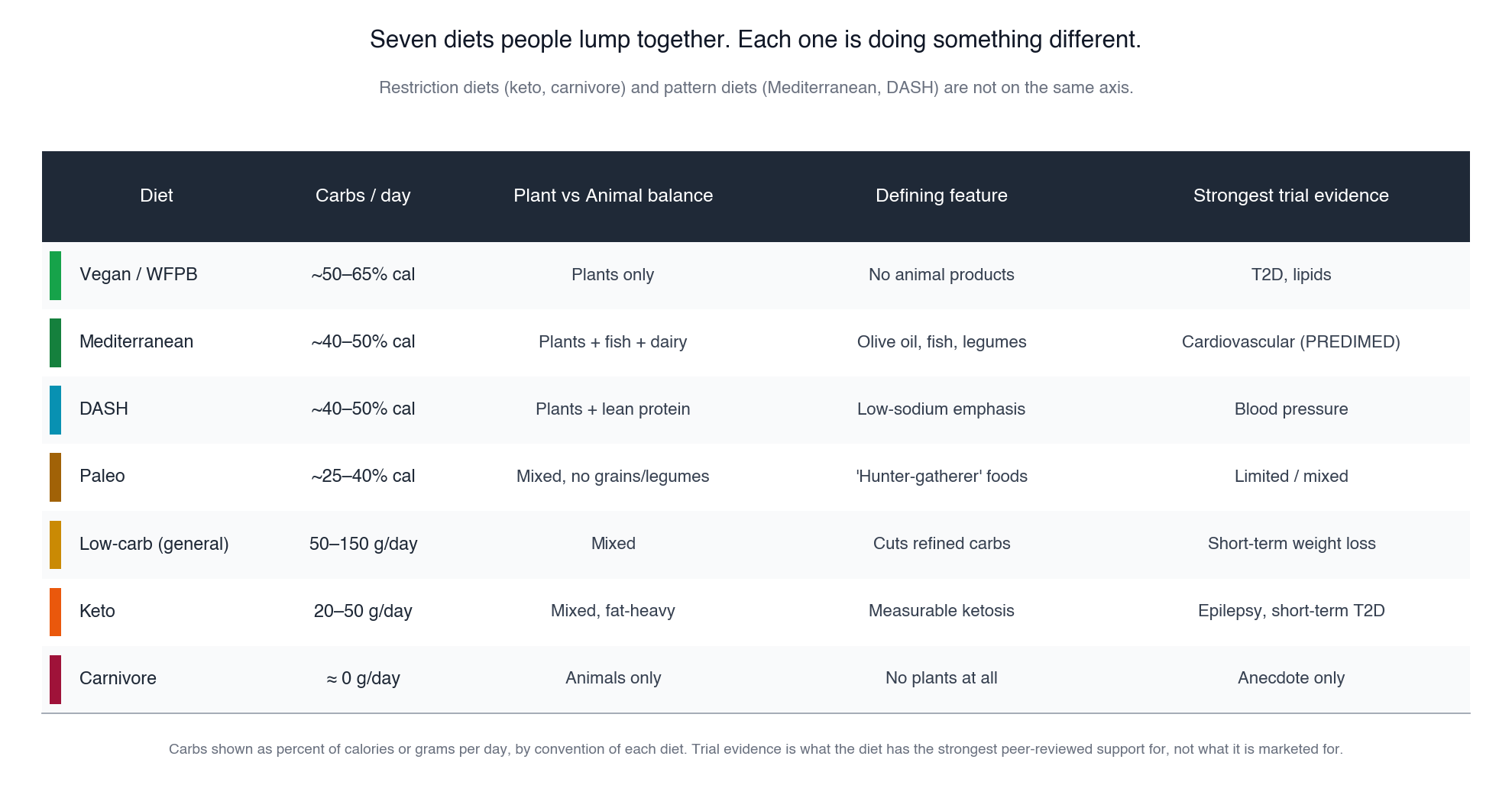
Low-carb, in the loosest sense, means somewhere between 50 and 150 grams of carbs a day. Cutting bread, pasta, sugar. Keeping fruit, beans, starchy vegetables, often whole grains. This is what most people mean when they say “I cut carbs.” It does not require any particular metabolic state. Most “I’m cutting carbs to lose weight” experiments live here.
Keto is much stricter. Roughly 20 to 50 grams of net carbs a day, around 70 to 80 percent of calories from fat, moderate protein. The defining feature is that you push your body into measurable ketosis, where it burns fat for fuel and produces ketone bodies (chiefly beta-hydroxybutyrate) at levels above 0.5 mmol per liter. Real keto is metabolic, not just low-carb. The original use case, going back to the 1920s, was treating drug-resistant pediatric epilepsy, and that clinical use is still real today and lives in academic medical centers, not on Instagram.
Carnivore is the strictest sibling. Only animal products. Strict carnivore is meat, salt, water. Paul Saladino’s animal-based version includes some fruit and honey. Mikhaila Peterson’s lion diet is ruminant meat only, no chicken or pork. Whether carnivore counts as keto depends on the protein-to-fat ratio, because high protein can blunt ketosis through gluconeogenesis.
These nest imperfectly. All carnivore is low-carb. Some carnivore is ketogenic. Most keto is low-carb. Low-carb is not always keto.
What about Mediterranean and DASH?
This is the question worth pulling apart, because Mediterranean and DASH are not on the same axis as keto. They are a different framework entirely.
Keto, low-carb, and carnivore are restriction diets. They are defined by what you remove. Mediterranean and DASH are pattern diets. They are defined by what you eat. Mediterranean leans on olive oil, fish, legumes, leafy vegetables, whole grains, modest dairy, occasional poultry, very little red meat. DASH is the blood-pressure-focused version developed at the NIH, with a similar plant-and-fish skeleton plus an explicit sodium target. Both have around 40 to 50 percent of calories from carbs. Both are evidence-rich. PREDIMED, the big Mediterranean trial out of Spain, randomized 7,447 high-risk adults and showed roughly a 30 percent reduction in major cardiovascular events on Mediterranean compared to a low-fat control. DASH was developed specifically to lower blood pressure and does so reliably in trials.
You can do keto and Mediterranean simultaneously in principle. Olive oil, fish, leafy greens, skip the grains and legumes. But the standard versions of these patterns are not low-carb. They have more in common with each other than with anything in the keto family.
Where the evidence actually sits
The keto family has a few real wins and a lot of mixed-to-negative.
Pediatric refractory epilepsy: clinical keto works and has worked for a century. That clinical use is not the same thing as the influencer version.
Type 2 diabetes, short to medium term: keto reliably drops glucose, A1C, and insulin requirements. Virta Health’s five-year follow-up studies show meaningful diabetes remission rates with intensive support. The catch is adherence.
Weight loss: keto causes weight loss, and so does every other restrictive eating pattern. Head-to-head trials of keto versus low-fat versus Mediterranean find roughly similar long-term weight loss at one to two years. The mechanism is mostly calorie reduction, helped by protein satiety.
Cardiovascular disease: the contested zone. Some people, especially lean, healthy adopters of keto, see large LDL and ApoB increases on the diet. The “lean mass hyper-responder” phenomenon. Whether that elevated LDL on keto carries the same atherosclerotic risk as elevated LDL otherwise is the open question, and it is where keto’s most-cited “high LDL on keto is fine” study, the 2025 KETO-CTA paper, was retracted in March 2026 for selective reporting and unblinded CT reads. So the evidence base on this specific question is actively contracting, not expanding.
The Mediterranean and DASH evidence bases dwarf anything keto has produced for cardiovascular outcomes. That is not a bias against keto. It is the actual literature.
What I actually did
I do not do keto. I do not measure ketones. I track with MacroFactor and picked the “high-carb, low-fat” programme, because I like fruit and grew up in the 80s, when fat was still the source of all dietary evil. Old habits. I eat roughly 250 grams of carbs a day, mostly from fruit, dairy, beans, oats, and the occasional sourdough. I aim for plenty of protein, around 1 gram per pound of bodyweight, mostly from poultry, Greek yogurt, and steak. I work out five times a week (lifting plus indoor cycling and rowing). The drug, tirzepatide, did most of the hard work on appetite. The protein and the training protected lean mass on the way down. I’m also on TRT, which I’ve written about separately and which plays its own role in body composition at 53. The result is 170 pounds off and holding, with a body composition I have not had since my twenties.
When the next person asks me if it’s keto, I will tell them no. They will probably ask if it’s intermittent fasting. I will tell them no again. The right question, almost always, is “what changed?” Not “which diet?”
I keep a running tracker of every GLP-1 and incretin drug, approved and still in the pipeline, with what each one targets, how far along it is, and what's coming next.
See the full GLP-1 Pipeline Tracker →About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.