

I walked into our kitchen last week and saw a pink tub of Viactiv chews next to the coffee maker. My wife picked them up at the store on her own. Nobody told her to. She wanted to do something for her bones, and calcium chews are the obvious first move when that’s the goal.
I get it. Every CVS, every Walgreens, every pharmacy aisle in America stocks a wall of bone-support supplements. Plenty of women in America take some form of calcium, vitamin D, or both. For decades the working assumption was: it probably helps, and at worst it doesn’t hurt, so why not.
A lot of these come in chew, gummy, or chocolate form now. They feel less like medicine and more like a small treat that happens to be virtuous. The Viactiv on our counter is caramel-flavored.
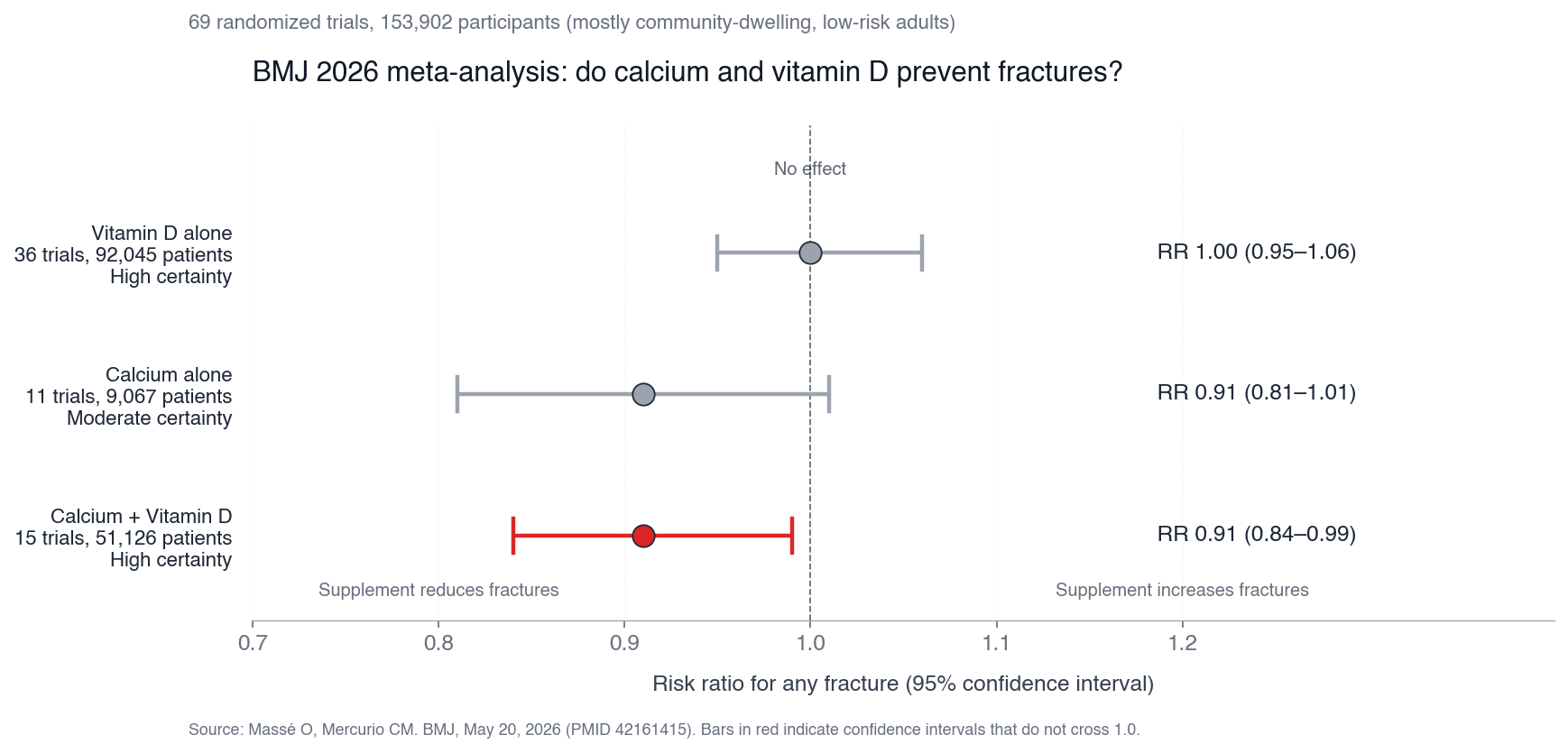
Then on May 20, BMJ published a new systematic review. 69 randomized trials. 153,902 patients. Mostly community-dwelling adults, not nursing-home residents or people with documented osteoporosis. The exact demographic that walks into a CVS and grabs a tub of Viactiv. The authors’ conclusion, in their own words: “little to no benefits from use of calcium, vitamin D, or combined supplementation on the prevention of fractures and falls.”
This is not biohacker advice. This is mainstream medicine.
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
I want to be careful here because the obvious response to a finding like this is “well, I never thought those worked anyway.” But the recommendation to take calcium and vitamin D for bone health did not come from Joe Rogan or the wellness internet. It came from primary care doctors, OB-GYNs, the National Osteoporosis Foundation, decades of clinical practice. The reason calcium chews and vitamin D gummies sit at eye level at the pharmacy is because doctors have been telling women to take them.
The US Preventive Services Task Force actually backed off this advice years ago. In 2018 they concluded the evidence was insufficient to recommend calcium plus vitamin D for primary prevention in healthy community-dwelling adults. But the message never really reached the average pharmacy customer, and most prescribing pads kept on going. The BMJ paper lays out cleanly why USPSTF had the right idea.
What 153,000 patients actually showed
The reviewers broke the trials into three arms. The vitamin-D-alone arm was the biggest: 36 trials, 92,045 patients. Risk ratio for any fracture came out at 1.00, with a tight confidence interval. Zero effect. The reviewers rated their certainty as high, which is academic-speak for “we are not coming back to this question.”
The calcium-alone arm was smaller: 11 trials, 9,067 patients. Risk ratio 0.91, hinting at a 9% reduction, but the confidence interval crossed 1.0. Not statistically significant. The combined-supplementation arm covered 15 trials and 51,126 patients, with a risk ratio also at 0.91 and an upper bound at 0.99, so it just barely clears the bar.
That last number is the most generous reading of the data, and even there the authors’ own framing is “little to no benefit.” Why? Because the absolute reduction in a low-risk population is tiny. If your 10-year fracture risk is around 4%, a 9% relative reduction takes you to 3.6%. You’d need to treat hundreds of people for years to prevent one fracture. And vitamin D alone, which is what most pharmacy customers are actually buying, did nothing.
Who this paper isn’t about
The population was 87% community-dwelling and 73% not at high fracture risk. So this is not a paper about people who already have osteoporosis or who fell last year and broke a wrist. Those populations have separate evidence and separate drugs. Bisphosphonates like alendronate, denosumab, romosozumab, and parathyroid-hormone agents have real benefits in established osteoporosis. That didn’t change on May 20.
The paper also doesn’t speak to dietary calcium from food. Eating Greek yogurt, sardines, dark leafy greens, and fortified plant milk is not the same intervention as swallowing a pill, and the trials only tested the pill. Food calcium comes with magnesium, vitamin K, and protein, all of which independently support bone density. Pill calcium comes alone. “Get your calcium from food” has been the cleaner advice for years, and this paper doesn’t disturb it.
And vitamin D in someone with documented deficiency, particularly people with very limited sun exposure or malabsorption, is a different question than vitamin D in someone whose level is already 30 ng/mL. The paper tested broad supplementation in mostly-replete populations. If you don’t know your level, that’s where to start, not at the supplement shelf. The blood test is cheap and tells you whether there’s any point.
What my wife pointed out
When I told my wife about the paper, she had two reactions. The first was the right question: “doesn’t vitamin D have other benefits?” The second, more emphatic: “also, they’re yummy.”
The other-benefits question is fair, and it’s the one most defenders of these supplements lead with. Vitamin D supposedly supports immune function, mood, cardiovascular health, cancer prevention. So even if it doesn’t move fractures, isn’t it doing something useful?
The biggest randomized trial we have on this is VITAL, published in the New England Journal of Medicine in 2019. 25,871 participants, five years, 2,000 IU of vitamin D3 daily versus placebo. Primary endpoints were cancer and cardiovascular events. Neither moved. Later substudies looked at depression, atrial fibrillation, and falls. The supplementation arm did not beat placebo on any of those either. There’s a hint of benefit on advanced cancer in a subgroup analysis, and some signals in specific populations, but the broad “give everyone vitamin D and watch the disease curves bend” story has not held up in the largest trial we’ve run.
Correcting a documented deficiency matters. (Which she has had in the past.) Flooding already-sufficient people with extra D mostly hasn’t moved the dial on the outcomes we care about. The BMJ paper is the bone-specific version of a pattern we’ve seen across endpoints for a decade.
And on the yummy point. She’s right. The caramel is doing more for the morning than the calcium, and there’s a real argument that a daily ritual you enjoy is worth something, even if the active ingredient is a wash. I’m not going to dispute that.
What probably does help your bones
The interventions with the strongest evidence for bone density and fracture prevention in normal-risk adults are unglamorous.
Strength training. Heavy resistance training, two to three sessions a week, builds bone density at the hip and spine in postmenopausal women. The LIFTMOR trial out of Australia showed measurable BMD gains in women with low bone mass doing supervised heavy lifting. This is the closest thing to a free lunch in bone health.
Weight-bearing impact exercise. Walking, jogging, jumping, hiking. The mechanical load on your skeleton is the signal your bones use to decide whether to maintain density. If you sit all day and never load your skeleton, no amount of calcium will fix that.
Adequate dietary protein. Around 1.2 grams per kilogram of body weight per day for adults over 50. Protein is structural for bone the same way it is for muscle.
Calcium from food, hitting roughly 1,200 mg a day for women over 50. Dairy, sardines, kale, broccoli, fortified soy or almond milk. Easier than people think.
Vitamin D from sun, food, and supplementation only if a blood test confirms you actually need it. I’ve written before about how cheap and informative the basic labs are. A 25-hydroxy vitamin D level tells you in one number whether to buy a bottle of D3.
DEXA scan to know where your bones actually stand. If you’re 50 and have never had one, that’s the actionable next step, not buying more chews.
What I’d do
I’m not going to tell my wife to throw out the Viactiv. The dose isn’t harmful, she likes how they taste, and the decision is hers. But if she asked me whether they were doing what the label suggests, I’d say no. The evidence that supported calcium and vitamin D supplementation for general bone health has been quietly dismantled over the last decade, and the BMJ paper is the cleanest summary of where we are now.
What I’d suggest, alongside or instead of the chews: more strength training, a DEXA at her next physical, and getting most of her calcium from food. The squat rack in the garage is doing more for her bones than anything that comes in a pink tub. If she keeps eating the chews because they’re delicious, that’s its own reason. Just not the one on the label.
h/t Eric Topol’s Substack note for surfacing the paper.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.