

I have been trying to figure out what “functional health” actually means for about a month, and the first thing I noticed is that the people selling it cannot agree on the term. The same business model gets called “functional medicine,” “functional health,” “root-cause medicine,” “integrative medicine,” and “personalized medicine” by practitioners who all want you to believe they are doing something different from your primary care doctor. Sometimes they really are doing something different. Often they’re doing the same thing under a different brand, sometimes worse and at higher prices.
This matters because the cultural moment is loud. Mark Hyman’s company Function Health closed a $298 million Series B round in November 2025 at a $2.5 billion post-money valuation, led by Redpoint Ventures with a16z and Battery alongside. Casey Means, who completed the Institute for Functional Medicine’s foundational coursework in 2019, is Trump’s nominee for Surgeon General. The new MAHA political coalition treats functional medicine as institutionally legitimate, with Hyman making the case directly on shows like The Megyn Kelly Show. My friends my age are paying for it, doctor friends are getting questions about it, and my Reddit feed is full of people asking why their functional medicine practitioner sent them home with a $3,000 supplement bill and no diagnosis.
So I looked at the documents, the academic critiques, the patient forums, and the financial filings. What follows is the cleanest version of what I found. Where the literature is contested I will say so. Where I am unsure I will say so. And where the model fails its users in documented, specific ways, I will name names.
Functional medicine’s one official definition is vaguer than it sounds
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
The Institute for Functional Medicine, headquartered in Federal Way, Washington, is the closest thing the movement has to a governing body. Its official definition runs like this:
“Functional medicine restores healthy function by treating the root causes of disease. The functional medicine framework allows clinicians to systematically identify and address the underlying processes and dysfunctions that are causing imbalance and disease in each individual. By understanding a patient’s genetic, environmental, and lifestyle influences, functional medicine clinicians create personalized interventions that restore balance, health, and well-being.”
I read that a few times and kept asking the same question: what, specifically, are they promising? They don’t name conditions or methods. They don’t name tests or treatments. There’s nothing in the definition you could measure outcomes against. “Root causes,” “underlying processes,” “imbalance,” “personalized interventions,” “balance, health, and well-being.” Every phrase in there could describe what your internist does, or what a chiropractor does, or what a wellness coach with no clinical training does. The definition is a tent that fits anyone who wants to stand inside it.
The institutional anchor is the Cleveland Clinic Center for Functional Medicine, opened in 2014 with Mark Hyman as founding director. Cleveland Clinic is a serious hospital. Lending its name to a center for functional medicine gave the movement institutional cover the way Harvard’s name does for almost any program with “Harvard” in the title. Hyman left around 2020 to focus on Function Health and other ventures, but the center remains. Its public-facing site is striking in what it does not say. There are no clinical-trial-level outcome claims for any specific condition. The marketing is built around “food as a first-line therapy” and lifestyle counseling delivered in a literal premium wellness building (yes, the building itself is part of the marketing). Patient examples are 10-week wellness programs. That is not a description of medicine; that is a description of a premium concierge service that uses medical credentialing as cover.
The certification picture matters here, because it is the part most laypeople misread. The IFM created the International Board of Functional Medicine Certification (IBFMC), and it offers two credentials. One is the Functional Medicine Certified Professional, available to nurses, nutritionists, and chiropractors within their scope of practice. The other is the FMCP-M, available to physicians, nurse practitioners, physician assistants, and naturopathic doctors. That last category is where this gets messy. The IFM bundles naturopaths together with MDs and DOs as if the credentials were equivalent in scope of practice. They are not. A naturopath who completes IFM training can present themselves as a “board-certified functional medicine physician” with the same credential string as an actual MD, and most patients have no way to tell the difference.
The other thing patients don’t know is that the IBFMC is not on the American Board of Medical Specialties roster. ABMS is the actual gatekeeper for medical specialty certification in the United States. Internal medicine, cardiology, family medicine, dermatology, all those go through one of the 24 ABMS member boards. The IBFMC is a self-established board by the same organization that runs the training. The seal looks real enough to a patient who has never had reason to look up what an ABMS board is, which is most patients.
Patients see a legitimate-looking seal and assume MD-level training is behind it. Often it isn’t.
Function Health is the $499-a-year consumer face of the movement
Function Health launched in 2022. Mark Hyman is the chief medical officer. The company is the cleanest commercial expression of functional medicine I have found, in the sense that you can describe the product in three bullet points without losing what it sells.
A subscription is $499 a year, HSA/FSA eligible, with a $365 first-year promotional rate. The membership covers a biomarker panel of around 160 lab tests pulled twice a year, organized into five categories on the dashboard: hormones and thyroid, “cancer and silent risks,” heart and metabolic, aging, and “mental health and focus.” MRI, CT, and mold-reactivity testing are paid add-ons. The “cancer and silent risks” category includes Grail’s Galleri multi-cancer early detection test. Function’s marketing pitches this as monitoring “early indicators of 1000s of diseases.”
My take, after living with the panel for a while.
The labs are real. Most of what’s on the panel is the same complete blood work a careful preventive physician would order if you asked. ApoB, Lp(a), fasting insulin in addition to glucose, hs-CRP, HbA1c, a real thyroid panel beyond TSH, sex hormones, ferritin, vitamin D. American primary care still doesn’t routinely pull ApoB or Lp(a), and those are the lipid markers that actually predict cardiovascular risk over the long arc. Fasting insulin tells you about metabolic dysfunction before HbA1c does. A real thyroid panel catches things TSH-alone misses. Function didn’t invent any of this. It packaged evidence-based markers preventive cardiology has been pushing for the last decade and put them behind a clean dashboard. If you’d be paying out of pocket for the labs anyway, the math works.
The part I’d skip on the dashboard is the “mental health and focus” category. There are no validated lab markers for depression, anxiety, ADHD, or any of the things 36 biomarkers are supposed to be measuring. Vitamin D, B12, thyroid, and a few inflammation markers can flag secondary contributors. The category as branded is marketing taxonomy, not medicine.
The conflict of interest is the part I get stuck on. Hyman, as chief medical officer, is the same person who built a 30-year media empire on the claim that conventional medicine misses what functional medicine catches. The product and the polemic are run by the same person. That isn’t automatically disqualifying, lots of clinicians have product lines (Dean Ornish, Peter Attia). The pattern matters more when the person running the polemic has a documented history of overstating evidence. Hyman does.
The evidence base is one observational paper and a lot of testimonials
When functional medicine advocates get asked for evidence, they point at one paper. The paper is real. The criticisms are also real, and you don’t have to be a methodologist to see them.
Cleveland Clinic looked back at its own data and published a 2019 study in JAMA Network Open (Beidelschies et al., PMID 31651966). They compared 1,595 patients who had been seen at the Center for Functional Medicine to 5,657 patients seen at Cleveland Clinic’s regular family practices. They asked patients how they felt at 6 months and again at 12 months using a standard quality-of-life questionnaire. The functional medicine group reported a small improvement; the regular primary care group reported almost none. The numbers were statistically significant. The authors’ own concluding line is “Prospective studies are warranted to confirm these findings.”
David Gorski at Science-Based Medicine published a methodological critique a few weeks later, and his points hold up.
The study wasn’t randomized. Patients chose the functional medicine arm themselves. The people willing to pay out of pocket for boutique care were not the same baseline population as the people who walked into regular primary care. Self-selection is the simplest explanation for any difference in patient-reported well-being.
The outcome wasn’t lab values or hospitalizations or mortality. It was the answer to a survey question, scored on a 50-point scale. People who have paid thousands of dollars and spent 60 to 90 minutes per visit with their clinician will report feeling better. That is a well-documented effect of attention itself, not specifically of functional medicine.
The differences were small in absolute terms. Two points on a 50-point scale, even granting the comparison, is not the kind of effect that should change anyone’s practice. With a sample size that big you can hit statistical significance on almost any small difference. Clinical significance is a separate question and the paper does not address it.
They didn’t equalize visit length. American primary care runs 15 minutes per visit. Functional medicine runs 60 to 90. Give regular PCPs 90 minutes per patient and I doubt the gap survives the comparison. The follow-up paper Cleveland Clinic published in BMJ Open in 2021 doesn’t fix any of this. It compares group functional medicine visits to individual ones, both inside the same practice.
That single 2019 paper is what the IFM cites, what Function Health cites, and what Hyman points at when he gets challenged on evidence. There isn’t anything else at that level. There are case series, practitioner testimonials, and a great deal of marketing copy. There is no functional medicine RCT with a control arm that gets the same visit length and is measuring something objective. The absence isn’t automatically damning. Nutrition and lifestyle research is genuinely hard to randomize, and the rest of lifestyle medicine has the same problem. It does mean that when someone tells you functional medicine is evidence-based, they are pointing at one observational study and a lot of grateful customers.
Where the model breaks down
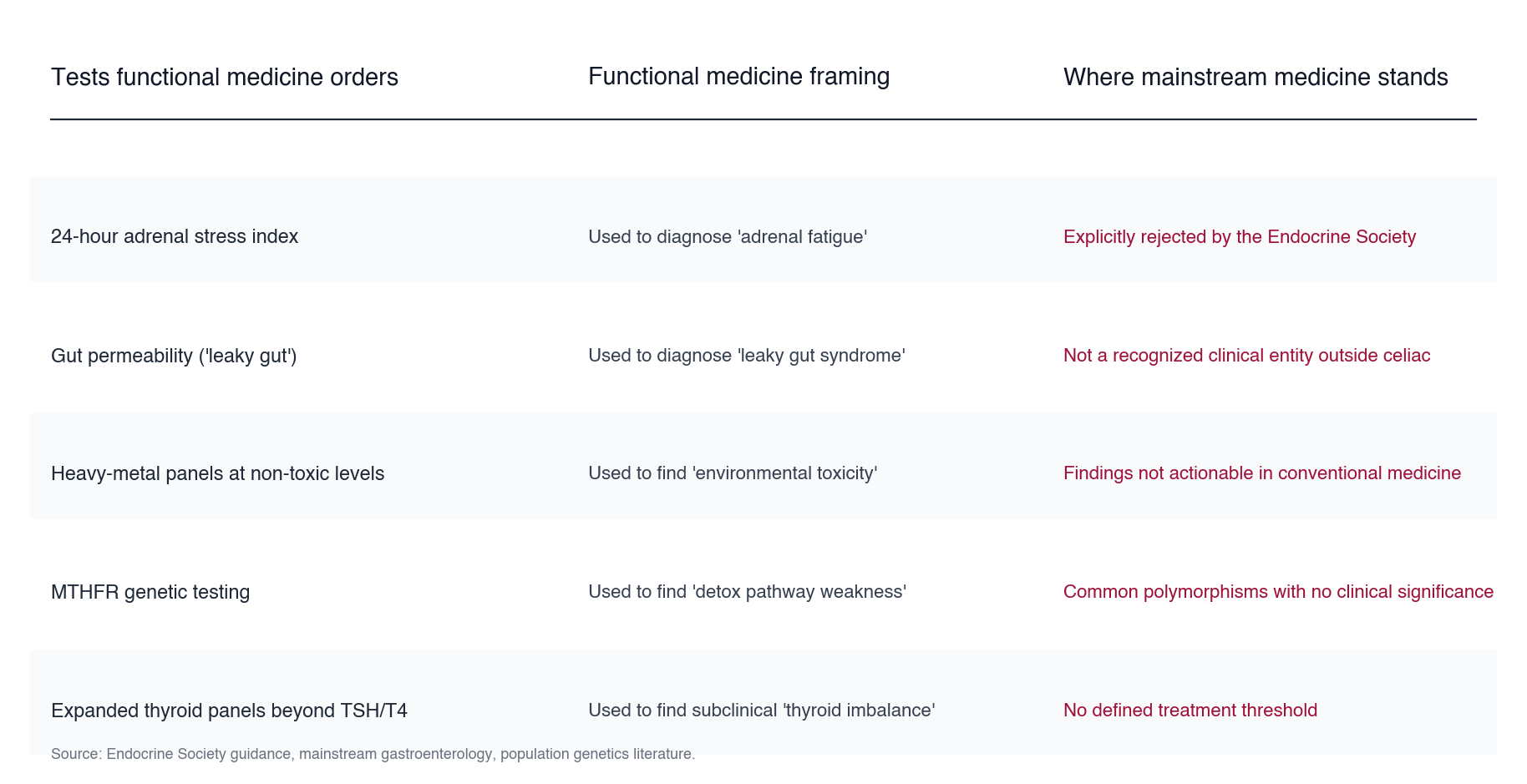
Functional medicine practitioners routinely order panels that the rest of medicine has either rejected or never adopted. The 24-hour adrenal stress index, used to diagnose “adrenal fatigue,” is explicitly rejected by the Endocrine Society. “Adrenal fatigue” itself isn’t a recognized diagnosis. Expanded thyroid panels beyond TSH and free T4 get ordered to find subclinical “imbalances” that have no defined treatment threshold, so the practitioner can prescribe something for them anyway. Gut-permeability tests claim to diagnose “leaky gut,” which outside of specific conditions like celiac disease is not a recognized clinical entity in mainstream gastroenterology. Heavy-metal panels run at non-toxic levels manufacture urgency around findings a conventional doctor would never act on. Genetic testing surfaces “MTHFR mutations” and “detox pathway weaknesses” that, in actual population genetics, are common polymorphisms without established clinical significance.
You buy the tests. Then the supplements the practitioner prescribes for whatever the tests turned up. Then another round of tests six months later. Gorski’s line for the pattern is “reams of useless tests in one hand, a huge invoice in the other,” and the line lands because it’s literally what the visits look like.
The supplements are not incidental to the model, they’re the revenue engine. Amy Myers, MD, sells The Myers Way® line at $43.97 to $57.97 per bottle. Will Cole, who is not an MD (his credentials are IFMCP, DNM, and DC), sells The Inflammation Spectrum® line. Hyman has been selling supplements through his own storefronts for nearly two decades. The lab testing exists in part to surface deficiencies a supplement can be sold to fix. Patients on r/functionalmedicine describe what this looks like in their own dollars: “$15,000 over three years” with no resolution; “I sunk about $3,000 and it was a total bust”; one quoted treatment plan for $65,000 for an 18-year-old with neurological symptoms. The subreddit itself carries warning posts from its own members: “Please do not work with the people who advertise themselves in these subs. They are not qualified and are working in a concerted effort to promote one person or program.”
There’s a darker failure mode, and this is the one that should make even the most charitable reader of functional medicine pause. Practitioners at the top of the movement promote interventions that have no evidence base, sometimes have explicit safety concerns, and sometimes nearly kill them.
The most recent example, documented in detail by the journalist Scott Carney, involves Mark Hyman. In November 2024, Hyman published a podcast episode titled “Stem Cells & Peptides: The Secret to Reversing Chronic Pain and Aging | Dr. Adeel Khan.” Hyman wrote his own show notes for the episode. The notes are preserved in third-party podcast caches, including the JSON-LD metadata at goloudnow.com. His own words: “I sit down with regenerative medicine expert Dr. Adeel Khan to explore cutting-edge approaches in functional medicine. From the power of stem cells and exosomes to cutting-edge gene therapy, discover how these therapies work to combat chronic pain, reverse aging, and enhance longevity. This isn’t science fiction, it’s the future of medicine.”
Adeel Khan operates regenerative medicine clinics in Mexico, Dubai, and Japan. None of the treatments he provides for the indications Hyman promoted are FDA-approved for those uses. The “engineered mesenchymal stem cells and mesenchymal exosomes injected epidurally” that Khan offers for spinal degeneration are explicitly the kind of treatment the FDA has issued warning letters about. Khan sets up in countries with loose cell-therapy rules and sells procedures that can’t be done legally in the US. That’s the business model.
Per Carney’s reporting, Hyman flew to Cabo for treatment and received an injection that, by Carney’s account, came from Khan. The injection got infected. The infection became sepsis. Hyman was hospitalized, had emergency spinal surgery, then a second surgery, and was told he was “maybe a couple of days away from dying.” He lost 25 pounds and could not walk, brush his teeth, or wipe himself for months.
Hyman has now spoken publicly about the incident on at least two podcasts, the August 18, 2025 Jay Shetty episode and a December 2025 follow-up. The verbatim transcript of the Shetty episode, which I transcribed via the Whisper API on May 22, 2026, runs 14,804 words. Across all 14,804 words, the audio contains zero mentions of “Khan,” zero mentions of “Adeel,” zero mentions of “stem cell,” zero mentions of “exosome,” and zero mentions of “regenerative medicine.” Hyman describes the incident this way:
“I ended up having an injection, which is a pretty common treatment to help relieve pain. And one of the risks of injections, if any at all, is infection. And in a closed space of the spine, it just took off.”
The November 2024 episode in which Hyman branded Khan as a “regenerative medicine expert” and his stem-cell injections as “the future of medicine” has been deleted from Hyman’s primary feeds. The Wayback Machine has no snapshot. Carney’s framing of the timeline, hedged as “likely gave the functional medicine doctor Mark Hyman sepsis,” is the carefully lawyered version. The documentary record supports him.
The founder of the most prominent functional medicine institution in the United States nearly died from a treatment he had personally promoted as the future of medicine three months before he received it. After his near-death experience, he publicly reframed the treatment as a routine pain injection and scrubbed the original promotional content from his own feeds. He has continued to platform the practitioner who provided the treatment on subsequent episodes, including a May 9, 2025 multi-guest episode that is still publicly available. None of this required private investigation to surface. Hyman’s own show notes, his own scrubbed audio, his own public statements after the fact are all sitting in plain view if you know where to look.
Not every functional medicine practitioner is reckless. But the founder-figure of the movement, by his own published words on both sides of his near-death experience, has demonstrated the specific failure mode the category is most vulnerable to. He was willing to promote an unvalidated treatment as routine medicine. He was unwilling to be straight about it when it nearly killed him. If the person at the top of the field operates this way, the rule of thumb for evaluating anyone below him writes itself.
What I would do
Skip the practitioner. Keep the labs.
A lot of American men in their forties and fifties would benefit from a more complete biomarker panel than their PCP runs by default, and Function Health is one viable way to get that panel. If you have the money and the dashboard is worth $499 a year to you as a self-tracking tool, the product works as advertised on the lab front. Use it the way you would use any blood-testing service. Get the numbers, take them to a physician who does evidence-based preventive medicine, and ignore the parts of the dashboard that are marketing.
What I wouldn’t do is pay $200 to $500 per visit to a functional medicine practitioner for advice that turns out to be mostly nutrition counseling, sleep optimization, and supplement upselling. Most of the genuinely useful interventions sold under the functional medicine banner are already mainstream preventive medicine at this point. Better protein and fiber intake, seven to nine hours of sleep, daily movement, two strength sessions a week, a complete blood panel including ApoB and Lp(a) and fasting insulin once a year. If something is off on the panel, work with a board-certified physician who can read the result against your full history. The functional medicine practitioner does not have specialty training your internist doesn’t.
The financial signature I would avoid is any practitioner whose treatment plan starts with $3,000 to $5,000 of mold-toxicity, heavy-metal, gut-permeability, or “comprehensive hormone” panels before any specific clinical question has been answered. That sequence is the operating model of the category at scale, not the failure of one bad practitioner.
What keeps nagging me is this. The most useful work functional medicine has done is push mainstream American medicine on lifestyle, nutrition, and preventive testing. That fight is mostly won at this point. ApoB-first lipid management is becoming standard. Earlier GLP-1 prescribing is becoming standard. CGMs outside frank diabetes care are moving in the same direction. Lp(a) screening is on its way. None of that requires a $499 subscription or a practitioner outside the ABMS system to access. What functional medicine still owns exclusively is the part of the package that should make you wary: the supplement pipeline, the manufactured diagnoses, the credential laundering, and the platforming of unvalidated treatments as if they were routine medicine.
Decide for yourself whether the parts you find useful are worth the parts you find dangerous. My read is the labs are worth $499 and the practitioners aren’t worth $200. If you’re not sure, watch what the people running the movement do when their own treatments nearly kill them. Watch what they say afterwards. The pattern is informative.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.