
What cholesterol actually is, before the numbers
Get the free Bloodwork Decoder
You just read how to make sense of a cholesterol panel. I put all of it, ApoB and Lp(a) included, into a one-page cheat sheet: what every number means, what to aim for at 50, and what to ask your doctor. Subscribe free and I’ll send it to your inbox. No spam, nothing to sell.
I have been getting my lipid panel done every few months for the past 18 months. Every time it comes back it has about a dozen numbers on it, and the first half-dozen times I had no idea which ones actually mattered.
This week the American College of Cardiology published the first major update to the cholesterol guidelines since 2018. The guideline is 134 pages of dense cardiology. The version that is useful to a fifty-year-old guy who wants to know what to do at his next physical is a lot shorter than that. This post is that version.
I am not a clinician. I am a guy who learned this stuff over the past two years because my own numbers needed it. I am going to walk through what cholesterol is, what the four numbers on your panel actually mean, what to aim for, what the drugs do, and what to do this week if you have not had your panel done in a while. The new guideline changed a few things that are worth knowing. I will flag those as we go.
Your body makes cholesterol on purpose. It is not a toxin. Every cell in your body has a membrane made partly of cholesterol. Your testes make testosterone out of cholesterol. Your liver makes bile salts out of cholesterol. Your skin makes vitamin D out of cholesterol when sunlight hits it. If you somehow eliminated all cholesterol from your body tomorrow, you would die before lunch.
The trouble starts when cholesterol gets transported around your bloodstream in the wrong containers, in the wrong amounts, for the wrong number of decades. Cholesterol does not dissolve in blood. Your body packages it inside small particles, the way you might wrap food in plastic to ship it. The particles have a fatty interior carrying cholesterol and triglycerides, and an outer protein shell that tells your liver and tissues what to do with the contents.
You have probably heard cholesterol described as “good” and “bad.” That is the bumper-sticker version of a real distinction. There is one cholesterol molecule. What changes is which particle is carrying it.
The two main particle families on a routine blood test are HDL and LDL. HDL particles ferry cholesterol from your tissues back to your liver for disposal. They are the cleanup crew. LDL particles deliver cholesterol from your liver out to your tissues. They are the delivery trucks. There is nothing inherently bad about a delivery truck. The problem is that when too many of them spend too many years driving past too many cracks in your arterial walls, they get stuck in those walls, get oxidized, attract immune cells, and over decades become atherosclerotic plaque. That is the plumbing version of what most heart attacks come from.
So when people say “lower your bad cholesterol,” what they mean in practice is “lower the number of LDL particles circulating in your blood for the longest time over the most years of your adult life.” Your panel measures the cholesterol carried inside those particles, which is a reasonable proxy. The newer numbers on the panel measure the particles themselves more directly. That is where ApoB comes in.
There is also one particle that behaves so differently from the rest that it gets its own line item: Lp(a). And there is a fourth family worth knowing about, called remnants. Remnant particles are bigger than LDL, they carry both triglycerides and cholesterol, and per particle they are roughly four times more atherogenic than LDL. Most people with overweight, insulin resistance, or visceral fat carry too many of them. I will come back to remnants in the numbers section, because the trick with them is that your panel does not actually print the number, but you can calculate it yourself for free.
The numbers on your panel
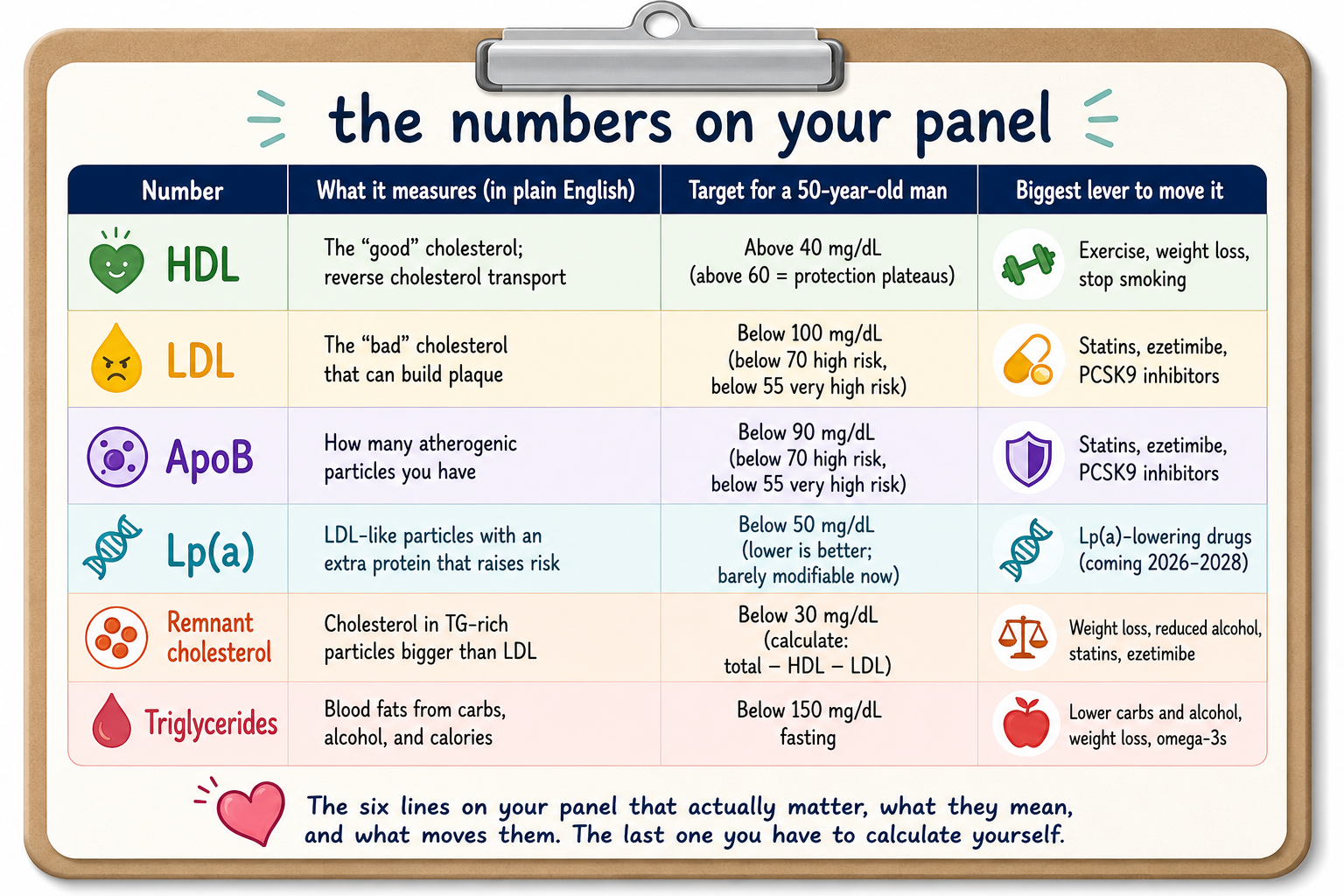
Your standard lipid panel reports four cholesterol-related numbers and a triglyceride number. I am going to walk through each in plain English: what it measures, and what number you actually want at fifty. I am also going to add a sixth number that does not appear on most panels but that you can calculate yourself.
HDL cholesterol. This is the cleanup-crew number, reported in milligrams per deciliter (mg/dL). Higher is generally better, but only up to a point. The bumper sticker says “high HDL is good.” The reality is that HDL is a marker for your overall metabolic health rather than a thing you should chase. Men with HDL above 40 mg/dL are doing fine. Men below 40 mg/dL have a clear cardiovascular risk increase. Above 60 mg/dL the relationship gets weird and the protection plateaus. There is no drug that reliably raises HDL and produces fewer heart attacks. So you measure HDL, you note where you stand, and if it is below 40 you treat it as one signal among several that your metabolic health needs work. You do not chase HDL with supplements or niacin. The trials that tried this did not pan out.
LDL cholesterol. This is the delivery-truck number, also in mg/dL. This is the number that drives most clinical decision-making. Higher LDL over your lifetime means more atherosclerotic plaque buildup. Lower means less. The relationship is monotonic, which is a fancy word for “as far as anyone has tested it, lower really is better.” The new 2026 guideline sets a goal of 55 mg/dL or below for several high-risk categories of patients. For the rest of us without established cardiovascular disease, the target depends on overall risk, but a reasonable rule of thumb is that 70 mg/dL is good, 100 mg/dL is acceptable but slightly worse over decades, and 130 mg/dL is starting to be a problem you should do something about. I will come back to the question of how low LDL should go, because the answer is more interesting than it sounds.
One catch worth knowing. The LDL number on your panel is usually calculated from total cholesterol, HDL, and triglycerides using a formula. The classic formula (called Friedewald) was developed in 1972 and gets less accurate when your LDL is already low or your triglycerides are high. The 2026 guideline now recommends using newer formulas (Martin/Hopkins or Sampson/NIH) as the default. If your LDL number looks suspiciously low while you are on a statin, ask your lab which formula they used.
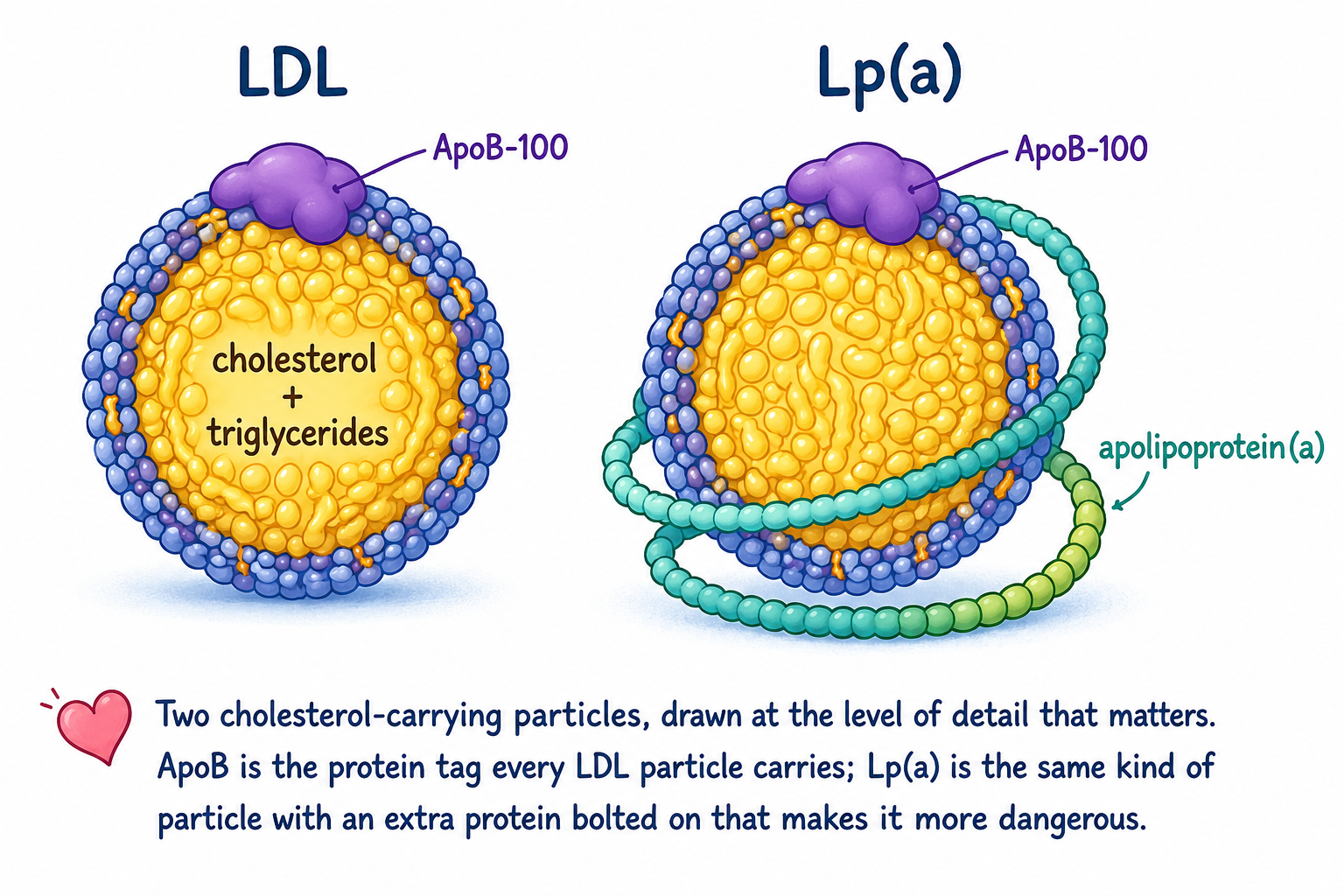
ApoB. This is the newer number you may not have on your panel, and the new guideline pushes for measuring it more often. ApoB stands for apolipoprotein B. It is the protein label on the outside of LDL particles and a few other atherogenic particles. Every one of those particles has exactly one ApoB molecule on its surface. So measuring ApoB gives you a direct count of how many atherogenic particles you have circulating in your blood.
Why this matters is that two people can have the same LDL cholesterol number and very different numbers of LDL particles. One person has fewer, larger particles carrying the same total cholesterol. The other has many, smaller particles carrying the same total cholesterol. The second person has higher cardiovascular risk because what damages your arteries is the number of particles knocking against the artery walls, not the total cholesterol weight inside them.
The 2026 guideline gives specific ApoB targets that line up almost identically with the LDL targets at each risk level. For someone at borderline to intermediate cardiovascular risk, ApoB below 90 mg/dL is the goal. For someone at high risk, below 70 mg/dL. For someone at very high risk (established cardiovascular disease with multiple events or major risk factors), below 55 mg/dL. The pattern is clean: whatever your LDL target is in milligrams per deciliter, your ApoB target is roughly the same number.
The guideline now formally recommends ApoB measurement in adults who are already on cholesterol-lowering medication, particularly if they have diabetes, kidney disease, or high triglycerides. This is the first US guideline to include ApoB as a measurement recommendation, and it is intentionally selective rather than universal. If you are on a statin and your LDL is at goal but you have not had your ApoB checked, ask.
Lp(a). This is the one that almost nobody measures and the 2026 guideline says everybody should measure once. Lp(a) is a specific type of LDL particle with an extra protein bolted on (apolipoprotein-little-a). It accelerates plaque formation faster than regular LDL and makes your blood more prone to clotting. Your Lp(a) is essentially set by your genes. Diet, exercise, and statins barely move it.
About one in five adults has an Lp(a) level high enough to materially change their cardiovascular risk. Almost none of them know it, because almost nobody is testing. The 2026 guideline now says every adult should have it measured at least once for cardiovascular risk assessment, and this is the strongest possible class of recommendation. This is a one-blood-draw, once-in-your-life test, and the result does not change with the seasons or the diet you tried last summer.
For thresholds, anything above 50 mg/dL (also reported as 125 nmol/L on particle-based labs) is the risk threshold. At that level, your cardiovascular risk is about 1.4 times the population average. At 100 mg/dL (250 nmol/L), the risk roughly doubles. And per particle, Lp(a) is markedly more atherogenic than ordinary LDL, which means it does damage out of proportion to the cholesterol it carries. I wrote a longer post about Lp(a) three days ago if you want the deep version.
There is one tricky bit worth knowing. Your LDL cholesterol number on a routine panel actually includes the cholesterol carried inside Lp(a) particles. So if your Lp(a) is high, some of what your panel calls “LDL” is actually Lp(a), and lowering LDL with statins or ezetimibe will not touch that fraction. Two people with the same measured LDL of 80 mg/dL can be a meaningfully different cardiovascular risk if one has Lp(a) of 10 and the other has Lp(a) of 100. This is one reason ApoB and Lp(a) need to be measured alongside LDL, not assumed.
Remnant cholesterol. This is the number that does not show up on most lab reports but that you can calculate yourself from the lines that do. The formula is: total cholesterol minus HDL cholesterol minus LDL cholesterol equals remnant cholesterol. It costs nothing, requires no extra blood draw, and tells you whether you are carrying a lot of those particles I mentioned earlier that are bigger than LDL, carry both cholesterol and triglycerides, and are about four times more atherogenic per particle than ordinary LDL. The threshold most lipidologists flag is 30 mg/dL or above. Above that, you have meaningful residual cardiovascular risk even if your LDL is at goal. Remnants are particularly elevated in overweight, obesity, prediabetes, and chronic kidney disease, which is to say, in a large chunk of the audience reading this post. The 2026 guideline asks labs to report non-HDL cholesterol but stopped short of asking them to print remnant cholesterol, which is a missed opportunity. Do the subtraction yourself.
Triglycerides. Briefly, because they are on the panel and they matter, but they get less attention than they should at fifty. Triglycerides are fats that get packaged with cholesterol into VLDL particles. They are heavily diet-responsive. Above 150 mg/dL fasting is the soft threshold for elevated. Above 500 mg/dL is the pancreatitis-risk threshold. Above 1,000 mg/dL fasting, the new guideline says you should be referred to a registered dietitian. High triglycerides usually travel with metabolic syndrome, prediabetes, and visceral fat. They will move with weight loss and reduced alcohol intake more reliably than any other lipid number.
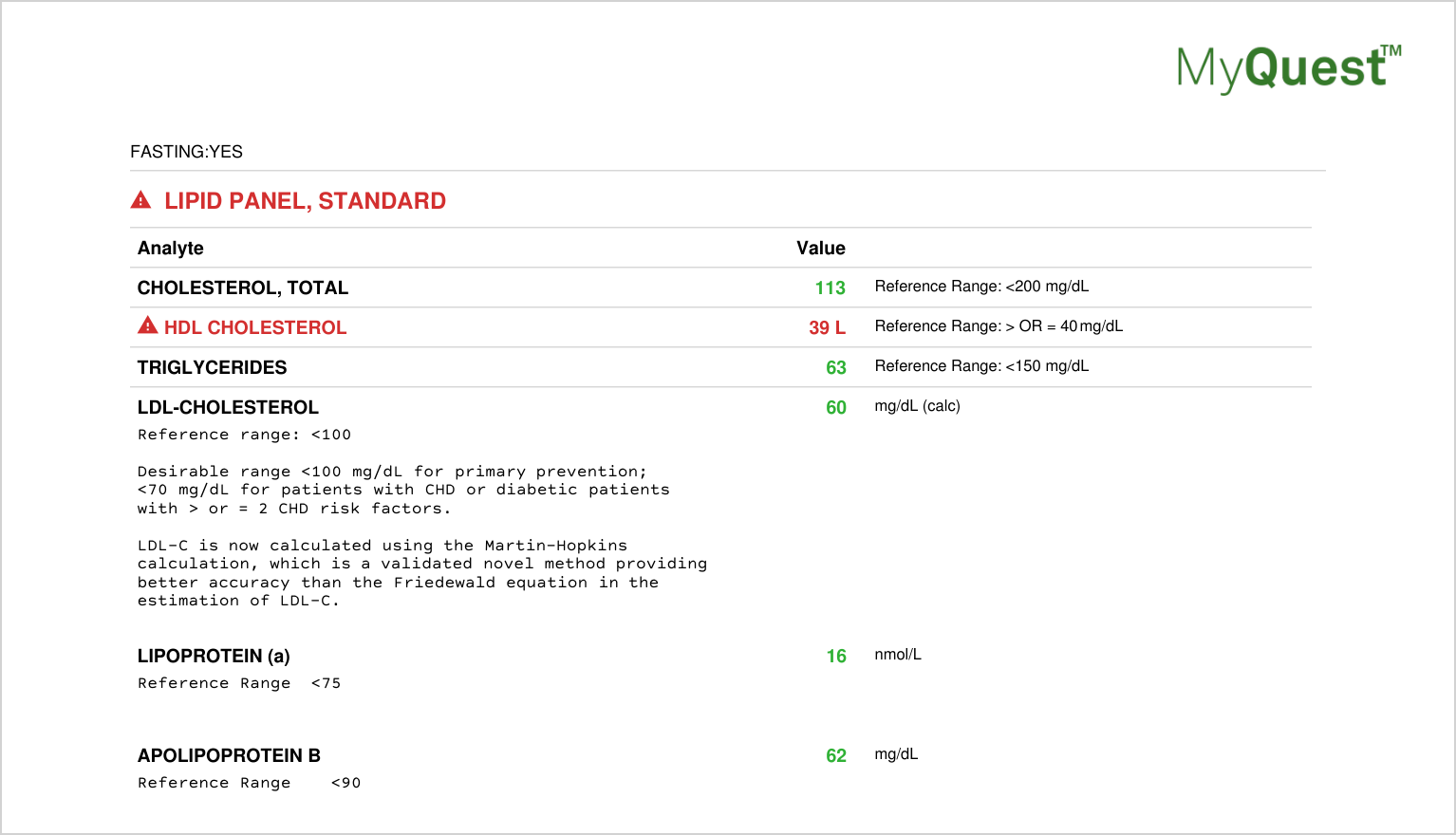
Here is what my own panel looked like at my last draw, May 2026.
- Total cholesterol 113.
- HDL 39, which Quest flags as low because the reference threshold is 40.
- Triglycerides 63.
- LDL 60, calculated using the Martin-Hopkins formula the new guideline now prefers, which my lab is already using.
- Remnant cholesterol works out to 14 (total minus HDL minus LDL), well below the 30 target.
- ApoB 62, below the 90 mg/dL optimal target and below the 70 mg/dL high-risk target.
- Lp(a) 16 nmol/L, well into the low-risk zone; i.e. I won in the genetic lottery.
One technically-flagged HDL, surrounded by clean numbers, in a guy only on ezetimibe and a GLP-1 who trains hard. It took a while to get here.
What the targets actually mean, and why “lower” is not always “better”
The headline finding of the 2026 guideline is that LDL targets are being pulled lower for more categories of patients. The number you will see is ≤55 mg/dL as the goal for high-risk groups. That is meaningfully tighter than where the previous guideline lived.
The natural question this raises is whether even lower would be better. The trials that drove this update do suggest that going from LDL of 90 to LDL of 40 with a PCSK9 inhibitor produces better cardiovascular outcomes than stopping at 90. So if 90 is worse than 40, would 30 be even better? Would 20?
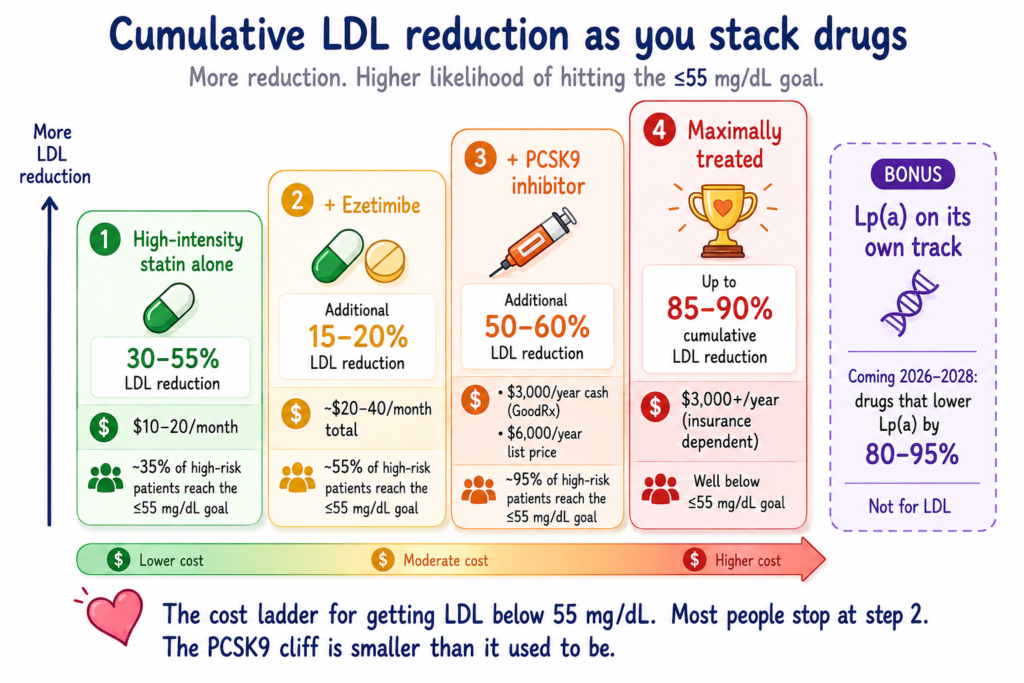
The honest answer from Gregory Schwartz, who wrote an editorial alongside the new guideline, is: probably yes biologically, but not necessarily in practice. The reason is cost and complexity. Most people with established cardiovascular disease can reach an LDL of 55 mg/dL with a high-intensity statin alone or, more commonly, a statin plus ezetimibe. Both are generic, costing roughly twenty dollars a month combined. To push LDL below 55 mg/dL, about 45% of patients would need to add a third lipid-lowering drug, typically a PCSK9 inhibitor. To push LDL below 30 mg/dL, more than 90% would need that third drug. PCSK9 inhibitors used to run about six to seven thousand dollars a year at list price, but the cash price for Repatha (the most-prescribed one) through GoodRx is closer to three thousand dollars a year right now, and insured patients with a copay assistance plan can pay single-digit monthly cost. The marginal cardiovascular benefit between an achieved LDL of 55 and an achieved LDL of 40 is, in absolute terms, small. The marginal cost still exists, but it is no longer the cliff it was on the original list price.
So the new guideline target of ≤55 mg/dL is the point at which the math stops favoring more aggressive therapy for most people. Whether your specific math favors going lower depends on your individual risk and what you can afford. If your Lp(a) is high and your family history is bad, you and your cardiologist might decide the marginal benefit is worth the cost. If you are a healthy fifty-year-old who hit 60 mg/dL on a statin and ezetimibe, you are probably done.
The 2026 guideline also tells your doctor to use a newer risk calculator called PREVENT, developed by the American Heart Association. PREVENT gives both a 10-year and a 30-year cardiovascular risk estimate, and it incorporates kidney function and metabolic factors that older calculators missed. You can run it yourself online for free with your last lipid panel, blood pressure, and a few other numbers from any recent physical.
The 30-year risk is the part most likely to change a conversation you have not had before. The guideline now says that adults aged 30 to 59 with a low 10-year risk (under 3%) should still be considered for statin therapy if either their LDL is 160 mg/dL or above, or their 30-year risk is 10% or above. The reasoning is what cardiology now calls “cholesterol pack-years,” analogous to smoking pack-years. The damage from elevated LDL accumulates by the decade. If you are 45 and your 10-year risk looks fine but your 30-year risk is 25%, the trial evidence says treating the LDL now is meaningfully better than waiting until you are 65 and the risk has caught up to you.
For a 50-year-old man, this matters in concrete terms. By age 55, about 95% of US men have a 30-year PREVENT risk of 10% or higher. The right reading is not that 95% of us need a statin tomorrow. It is that, at 50-plus, the conversation defaults to “should I be on lipid-lowering therapy” rather than “do I qualify for the conversation.” One of the editorial writers in the new guideline made an analogy worth keeping in mind: we do not tell a 40-year-old with blood pressure of 150 over 90 that treatment is unnecessary because his 10-year heart attack risk is low. The same logic now applies to LDL.
Coronary artery calcium scoring, the test that changes the conversation
There is one test the new guideline elevated that probably matters more than any single number on your lipid panel for a 50-year-old man, and most people I talk to have never heard of it. It is called a coronary artery calcium scan, usually shortened to CAC scoring. It is a low-radiation CT scan of your chest that takes about ten minutes, costs around a hundred dollars cash in most markets, requires no contrast dye, and gives back a single number that tells you how much calcified plaque you have in the arteries of your heart.
The intuition is straightforward. Calcified plaque is what atherosclerosis looks like once it has been there long enough to mineralize. Your lipid panel tells you what you are exposing your arteries to. Your CAC score tells you what has actually happened so far. Two men with the same LDL and the same age can have completely different CAC scores, and the one with more calcium has more disease, full stop.
The 2026 guideline upgraded CAC scoring to the strongest possible recommendation (Class 1) for men aged 40 and older with a borderline-to-intermediate 10-year risk on PREVENT. In plain English, the guideline now says: if you are 40+ and your calculator-based risk is in that middle band where the treatment decision is genuinely uncertain, get the scan. The scan resolves the uncertainty.
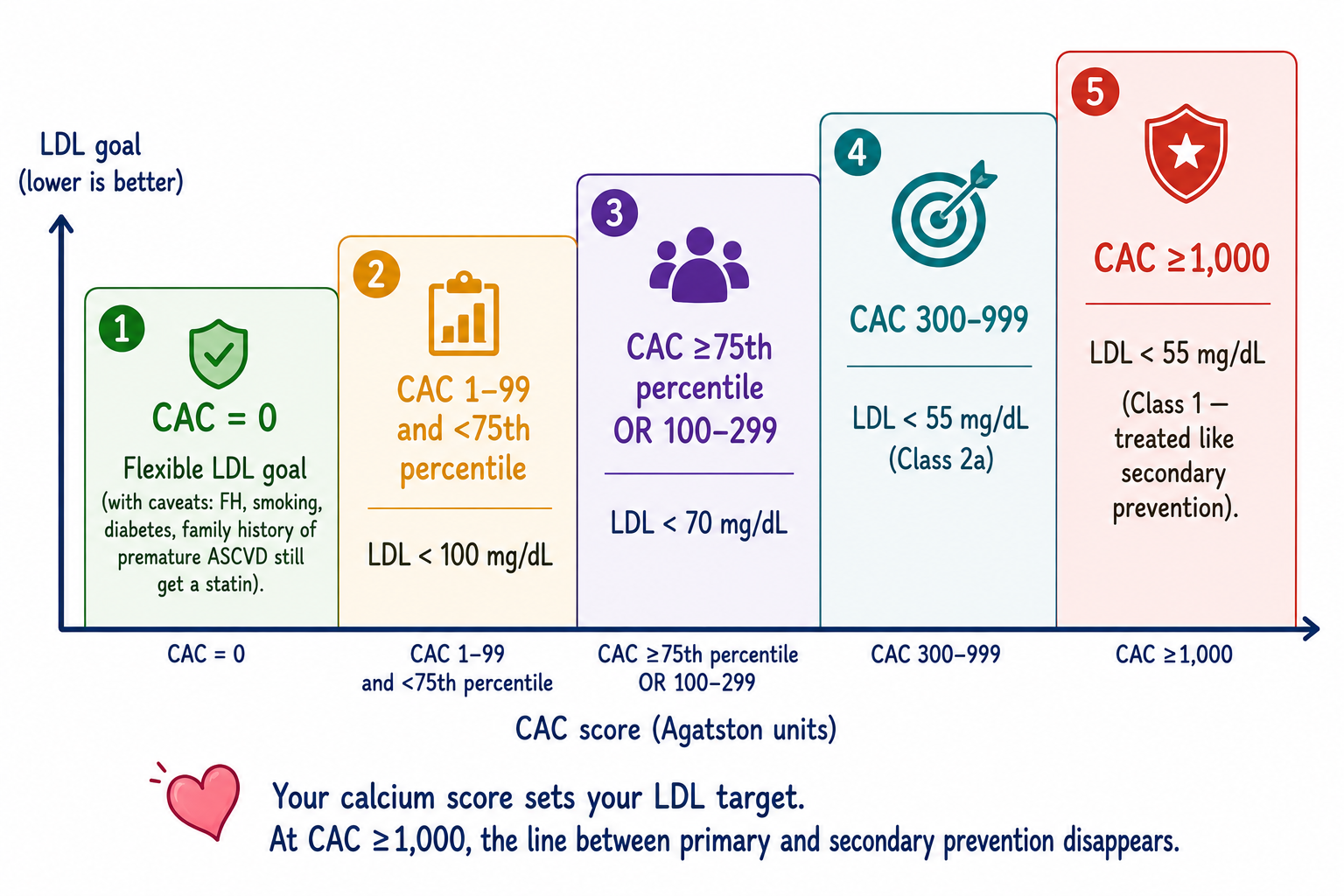
What the score means in practice. A CAC score of zero in a 50-year-old man is genuinely reassuring, and the guideline now lets your doctor flex the LDL goal upward if your score is zero (with a few exceptions I will get to). A score of 1 to 99 with you in the lower 75% of the percentile for your age means LDL goal below 100 mg/dL. A score at the 75th percentile or above, or 100 to 299, means LDL goal below 70. A score of 300 to 999 means LDL goal below 55. And a score of 1,000 or above means the guideline treats you the same as someone who has already had a heart attack. That last point is the one that should land: at a high enough CAC score, the line between “preventing your first event” and “preventing your second event” disappears.
The caveats matter. A CAC of zero does NOT excuse you from a statin if you have familial hypercholesterolemia, if you currently smoke, if you have diabetes, or if a first-degree relative had a heart attack before age 55 in men or 65 in women. In any of those four categories, the zero is not as reassuring as the population data suggests. The guideline writers specifically called this out.
One more useful thing the guideline did. If you have had a chest CT scan for any other reason in the past few years (lung cancer screening, a kidney stone workup, a COVID scan, anything), there is a good chance coronary calcium is already visible on those existing images, even if no one looked for it. The new guideline now treats moderate-to-severe coronary calcium incidentally seen on a non-cardiac chest CT as enough to drive an LDL goal of below 70 mg/dL. Translated: if you have had a chest CT in the past few years, ask your doctor to have the radiologist look at the coronaries and write up what they see. You may not need a separate CAC scan at all.
The drug classes, in plain English
There are six families of cholesterol-lowering drugs that matter for an adult man at fifty. Most people who need treatment use one or two. A small minority use three. Below is what each one does and what to know about it.
Statins. These are the workhorse, the cheap generic class, and the first thing your doctor will reach for. They block an enzyme in your liver that makes cholesterol. Your liver responds by pulling more LDL out of your blood to replace what it cannot make. Net effect: your LDL drops by 30 to 55 percent depending on which statin and what dose. Atorvastatin and rosuvastatin are the two high-intensity ones. They have been on the market for thirty years, cost almost nothing as generics, and have more long-term safety data than any other class of cardiovascular drug. They are, by any reasonable standard, one of the best buys in medicine.
The reason this matters is that statins are also the most-refused drug in cardiovascular medicine. About half of patients who get a prescription discontinue it within a year. The Editor-in-Chief of the journal that published the new guideline called this the single most important unsolved problem in cardiovascular prevention. Not the missing drug. The drug we have, that works, that people will not take.
Most of the reason people stop is muscle aches. And here is where the new evidence has gotten sharper than the old conversation around statins.
A new meta-analysis published this year (the Cholesterol Treatment Trialists Collaboration, looking at individual data from nineteen double-blind trials and about 124,000 patients) went through every adverse effect listed on statin product labels and tested whether the evidence actually supports it. Sixty-two out of the sixty-six listed side effects were not supported by the trial evidence. Statins did not cause memory loss. They did not cause depression. They did not cause sleep disturbance, erectile dysfunction, fatigue, headache, or peripheral neuropathy. The only confirmed harms beyond muscle symptoms and a small increase in diabetes risk were a small bump in liver enzymes and possibly some edema, both with absolute annual excess risks under 0.1 percent.
The muscle ache question itself has been studied head-on, and the result is worth knowing. In a study called SAMSON, patients who attributed muscle symptoms to their statin were taken through a sequence of blinded bottles, some containing the statin, some containing placebo, some containing nothing. About 90 percent of the symptom burden that patients had been blaming on the statin showed up identically when they were taking placebo. The symptoms were real. The cause was not the drug. This is called a nocebo effect, and it is one of the better-documented placebo-effect cousins in modern medicine.
What that does NOT mean is that you should ignore your own muscles. Some people genuinely do have a statin-related muscle response, and switching to a different statin or going to lower-but-more-frequent dosing usually resolves it. What it does mean is that the warning label on your statin overstates the case so far that the people most likely to benefit are the ones most likely to read it and refuse. The label is doing harm by accident.
Ezetimibe. A second-line generic that blocks cholesterol absorption from your gut. Adds another 15 to 20 percent LDL reduction on top of a statin. About twenty dollars a month. The 2026 guideline treats statin-plus-ezetimibe as the standard combination for patients who do not hit goal on statin alone. There is essentially no reason a patient who is not at goal on a statin should not try ezetimibe before reaching for a PCSK9 inhibitor.
PCSK9 inhibitors. Two flavors. The originals (evolocumab, alirocumab) are monoclonal antibodies given as an injection every two to four weeks. A newer entry (inclisiran) is a small interfering RNA given as an injection twice a year, and is now formally in the 2026 guideline. There is also an oral PCSK9 inhibitor (enlicitide) in late-stage trials that may be available in the next year or two. All of them work by removing a protein that destroys your LDL receptors, so your liver clears LDL out of your blood much more efficiently. Net effect: LDL drops by another 50 to 60 percent on top of a statin and ezetimibe. They are very effective and used to be very expensive. List price still sits around six thousand dollars a year, but the cash price via GoodRx for Repatha (the most-prescribed of these) is now closer to three thousand a year, and insured patients with a copay assistance plan can pay single-digit monthly cost. Inclisiran sits higher. The 2026 guideline reserves PCSK9 inhibitors for patients who cannot get to goal on statin plus ezetimibe, which is most people with established cardiovascular disease or severe genetic high cholesterol. The cost picture is meaningfully better than it was three years ago.
Bempedoic acid. A newer non-statin oral drug that works on the cholesterol-synthesis pathway as well, but only activates in your liver and not in muscle tissue, which is why it does not cause muscle aches. It is an option for patients who genuinely cannot tolerate statins. Lowers LDL by another 15 to 20 percent on top of whatever else you are on. About 350 dollars a month. Not first-line but worth knowing exists.
Lp(a)-lowering drugs. This is a class that does not yet exist as approved therapy but is the most exciting cardiology story of the next two years. Three drugs in late-stage trials (olpasiran from Amgen, pelacarsen from Ionis and Novartis, lepodisiran from Eli Lilly) lower Lp(a) by 80 to 95 percent. The Phase 3 outcome trials are reading out over the next 24 to 36 months. If they show that lowering Lp(a) actually reduces heart attacks in the way the genetics predict it should, the calculus for the one-in-five adults with high Lp(a) changes completely. Until then, the standard advice for high Lp(a) is to be aggressive about everything else you can control (LDL, ApoB, blood pressure, weight, sleep, smoking) because the drug that will lower the Lp(a) itself is still in trials.
Triglyceride and remnant-cholesterol drugs. This is a parallel pipeline most people will not need but that is worth knowing exists. For people with severe hypertriglyceridemia (fasting triglycerides above 1,000 mg/dL), the new guideline now formally recommends apolipoprotein C-III inhibitors, a class of drugs that drops triglycerides by 50 percent or more and reduces the risk of acute pancreatitis by roughly 80 percent. Beyond that, drugs targeting angiopoietin-like proteins are in late trials for the broader remnant-cholesterol-high population (triglycerides 150 to 500). Like the Lp(a) drugs, these are waiting on Phase 3 cardiovascular outcome trials to prove that lowering remnants actually lowers heart attack risk independent of LDL. For most people, this paragraph is “good to know”; for the small subset with familial hypertriglyceridemia or recurrent pancreatitis from triglycerides, it is the most important development in the new guideline.
What the lifestyle stuff actually does (and does not do)
The new guideline talks about lifestyle differently than the 2018 version. The word “obesity” appears 17 times in the 2026 guideline, versus twice in 2018. The phrase “physical activity” appears 31 times, versus 3. That is not an accident. It reflects a much better understanding of what is actually driving cardiovascular risk in the modern population.
For exercise, the guideline gives the strongest possible recommendation (Class 1) for a combination of regular aerobic exercise and resistance training in adults with dyslipidemia. Not “consider exercise.” Not “exercise is encouraged.” Recommended at the same level as a statin in someone who needs one. The honest reading of the trial evidence: exercise meaningfully lowers triglycerides and raises HDL, and it improves overall cardiovascular health through pathways the lipid panel does not capture (blood pressure, insulin sensitivity, vascular function, body composition). It also lowers LDL, but only modestly. The meta-analyses suggest about a 1.3 mg/dL drop in LDL per kilogram of weight loss in lifestyle interventions. Exercise and weight loss are necessary for cardiovascular health. They are not, on their own, sufficient to get a meaningfully elevated LDL into the new target range.
On diet, the 2026 Dyslipidemia Guideline gives a Class 1 recommendation to replace saturated and trans fats with monounsaturated and polyunsaturated fats, in the context of a diet that emphasizes fruits, vegetables, legumes, whole grains, nuts, and fiber. The specific thing worth flagging for a 50-year-old guy in 2026: the ketogenic and carnivore diets, increasingly mainstream in the men’s-health space, can raise LDL significantly in many people. If you are doing one of those diets and your LDL has gone up, that is not a coincidence and it is not a “metabolic advantage.” It is dose-responsive to the saturated fat you added.
The GLP-1 question comes up often because many of you are on Zepbound or considering it. The honest read on GLP-1 drugs and cholesterol: they lower triglycerides meaningfully (15 to 17 percent), lower LDL only modestly (5 to 8 percent), and the cardiovascular benefit they have shown in trials is much larger than the lipid changes alone can explain. In SELECT (the trial that demonstrated semaglutide reduces heart attacks and strokes in people with overweight and established cardiovascular disease), the LDL difference between arms was about 2 mg/dL, and the cardiovascular events dropped by 20 percent. The CV benefit of GLP-1 drugs is mostly NOT lipid-mediated. It is some combination of weight loss, blood pressure improvement, insulin sensitivity, direct vascular effects, and inflammation. So do not expect that starting Zepbound will get you off your statin. The two drugs are doing different things, and the new guideline keeps them in separate lanes.
A realistic plan at 50
Here is what to actually do. Four things, in order.
First, if you have not had a full lipid panel done in the past year or two, schedule one. Ask your doctor to include ApoB and Lp(a). ApoB will be covered automatically under the new guideline if you are on any kind of lipid medication or have diabetes or kidney disease. Lp(a) is a one-time test under the new guideline regardless of your situation. When the results come back, do the remnant cholesterol subtraction yourself: total minus HDL minus LDL. If that number is 30 or above, flag it.
Second, ask about a coronary artery calcium scan if you are 40 or older and your 10-year PREVENT risk lands in the borderline-to-intermediate range. If you have had any chest CT scan in the past few years for any other reason, ask the doctor to have the coronaries reviewed for calcium on those existing images instead. Either way, the calcium score is the test that turns a probabilistic risk estimate into a concrete picture of what is actually in your arteries.
Third, look at the whole panel and the calcium score in context. Your LDL number is meaningful, but not in isolation. Your ApoB tells you whether your particle count is consistent with your LDL number, or whether it is higher in a way the LDL number is missing. Your Lp(a) tells you whether your genes have loaded a meaningful cardiovascular risk you cannot see from the LDL alone. Your remnant cholesterol tells you whether your weight or metabolic status is loading risk on top of that. Your HDL is a marker, not a target. Your triglycerides reflect what you have been eating and drinking. Your calcium score tells you what has already happened to your arteries. Ask your doctor to run both the 10-year and 30-year PREVENT risk estimates. Take all of that to a doctor who actually reads it, ideally a cardiologist or a primary care doctor who has read the new guideline.
Fourth, treat the lipid panel as one input into a broader cardiometabolic picture. Blood pressure matters. Sleep quality matters. Visceral fat matters. Insulin sensitivity matters. The new guideline now explicitly puts cholesterol management in the context of cardiovascular-kidney-metabolic syndrome rather than treating lipids in isolation, which is a real shift from how this used to be framed.
If you have a first-degree relative (parent, sibling, or child) who had a heart attack or stroke at an unusually young age, men under 55 or women under 65, or if your own LDL has ever come back at or above 190 mg/dL, ask about genetic testing for familial hypercholesterolemia. The 2026 guideline recommends it in those scenarios, and a positive result changes both your treatment target and the conversation you should be having with your siblings and kids.
The guideline writers summarized the philosophy of the whole 2026 update in four maxims that I think capture it well. Screen earlier. Check regularly. Aim for lower LDL-C. Treat longer. The treatment that prevents your heart attack at 72 starts with the conversation you have at 52. The numbers above are the playbook in plain English. Take your panel in and have the conversation.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.
I’ve been reading and studying about metabolic health and cardiovascular health for several years and your summary here is the best I’ve read. Thank you so much for putting it together.