
A huge new Lancet study measured blood pressure and cholesterol in close to a million adults across seven countries. The finding that stunned me had nothing to do with Ozempic, and everything to do with the cheap, old-school drugs already sitting on the pharmacy shelf.
I take a weekly GLP-1, and I write about them constantly, so I expected the obesity news this month to be another chapter in the injectable story. It wasn’t. Instead, the paper that made me stop was about the decades before anyone took Ozempic for weight loss, and it hinges on a quiet point I keep forgetting. For two of the numbers that most decide your heart risk, blood pressure and cholesterol, a lot of the damage obesity used to do has already been blunted, and it was blunted by generics that cost about four dollars a month.
The study came out July 1 in The Lancet, from the NCD Risk Factor Collaboration, the group that tracks the world’s blood pressure and cholesterol. They pooled 110 national health surveys, close to a million people across England, the United States, Japan, South Korea, Taiwan, Thailand and Finland, from 1990 to 2024. The question was simple. Compare a person with obesity to a person at a normal weight, and see how far apart their blood pressure and their non-HDL cholesterol are, the second being the number that captures most of the artery-clogging particles, not just LDL. Then see how far apart those numbers were a generation ago.
The gap that used to define obesity has mostly closed
For adults over 40, the gap has nearly vanished. Older adults with obesity now walk around with blood pressure and non-HDL cholesterol that look about the same as their normal-weight neighbors, and in several countries a little better. The convergence was largest in the heaviest group, people with a BMI of 35 or more, which is exactly the group you would expect to be in the most trouble. Carrying a lot of extra weight is supposed to push those numbers up, and for decades it reliably did. On the two numbers doctors watch most, that link has quietly come apart.
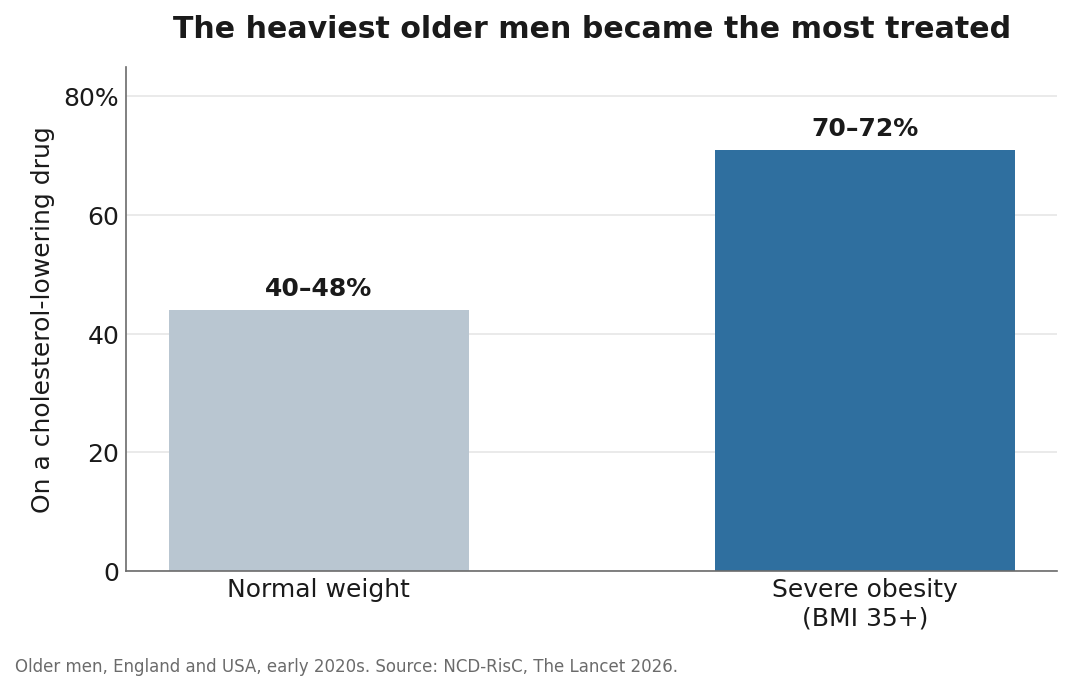
The authors are careful about why. This is an observational study, so it can show the pattern and point at the likely cause without proving it. Their explanation is not mysterious. Over the same years, people with obesity started taking a lot more cholesterol and blood pressure medication than everyone else. By the early 2020s, 70 to 72 percent of older men with severe obesity in England and the US were on a cholesterol-lowering drug, compared with 40 to 48 percent of normal-weight men. The heaviest people became the most medicated group, and their risk numbers came down to meet everyone else’s.
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
The drugs doing the work cost about four dollars
What is striking is how unglamorous the cause is. These gains came from statins and blood pressure pills, the kind of generic nobody builds a launch campaign around anymore. Medicaid’s own records show how cheap they got. By 2022, generics were 99.9 percent of statin prescriptions, and a generic fill ran about ten dollars, a fraction of what the brand-name versions had cost. Over those three decades, statin prescriptions in the program rose roughly fortyfold.
You can see the mechanism cleanly in an earlier US analysis. Between the early 1990s and the late 2000s, average total cholesterol in American adults fell from 216 to 197. Over the same stretch, the share of adults on a cholesterol-lowering drug went from 1.6 percent to 12.5 percent, while what people ate barely changed. The researchers estimated that the drugs, not diet, accounted for roughly half of the drop.
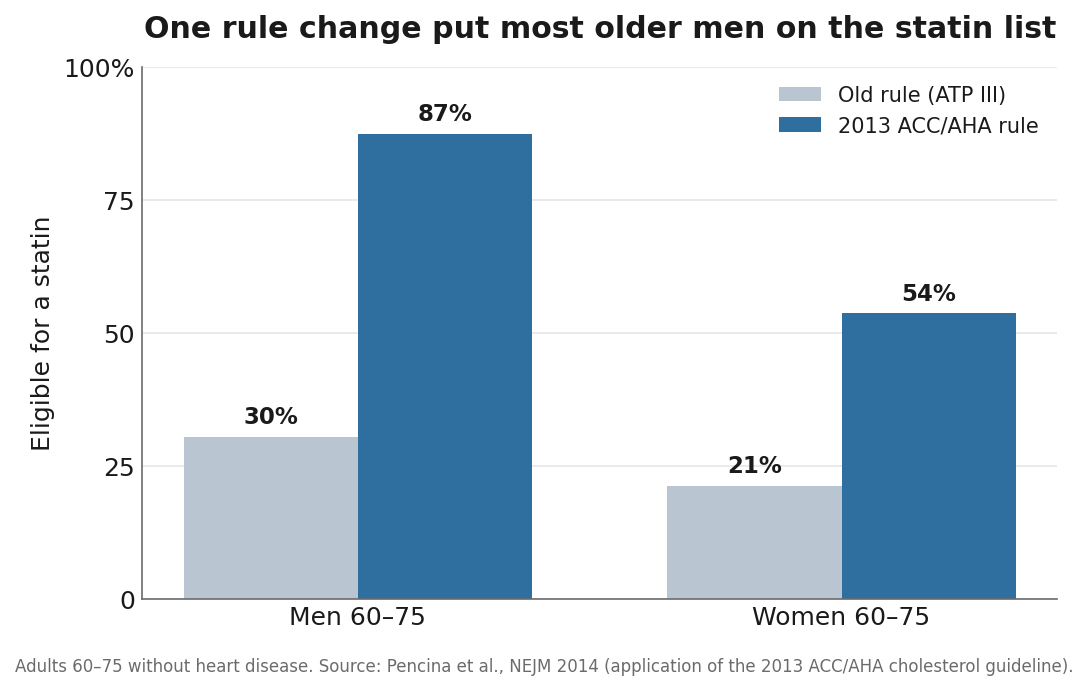
The other engine was a change in the rules. In 2013, the American College of Cardiology and the American Heart Association rewrote who qualifies for a statin, moving from cholesterol targets to overall heart risk. A study in the New England Journal of Medicine found the change made 12.8 million more American adults eligible overnight. Among men aged 60 to 75 without heart disease, eligibility jumped from 30 percent to 87 percent. The rule did not count obesity itself. It counted the things obesity travels with, higher blood pressure, diabetes, worse lipid numbers, and those feed the overall risk score. So once eligibility keyed on total risk instead of cholesterol alone, heavier people were more likely to cross the line onto treatment. The convergence in the Lancet paper is what that looks like a decade later, measured in a million people.
This trend is decades old, not a headline
When a finding surprises me, I check whether it is actually new or just newly packaged. This one is a continuation. US researchers saw it forming years ago, in JAMA work back in 2005 and again in NHANES data through 2010, as the tie between weight and these risk factors loosened while treatment spread. The Lancet paper’s contribution is scale and recency. It shows the trend held across seven countries, all the way to 2024, long enough to capture a decade of risk-based statin treatment in the US alongside similar medication trends elsewhere.
I find that reassuring in a specific way. You do not need to wait for the next molecule to protect your arteries. I take a blood pressure pill, telmisartan, and I keep a cuff on the kitchen counter, partly because my mother had high blood pressure and partly because I would rather know my number than guess at it. This study is a reminder that the routine is doing more than I give it credit for.
Who got left out
Two groups do not show up in the good news, and both matter.
The first is younger adults. Under 40, the gap between people with obesity and people at a normal weight has barely moved, because young adults rarely get put on these medications no matter what they weigh. The risk calculators that trigger a statin are built around your odds over the next ten years, and those odds look low at 30 even when your lifetime risk is high. So a heavy 30-year-old carries the old, untreated risk that a heavy 60-year-old has had medicated away.
That may be starting to change, and in a way that fits the whole story. In March 2026 the AHA and ACC rewrote the cholesterol guidelines again, and this time they bolted a thirty-year risk estimate onto the ten-year one. A thirty-year horizon is built to catch the young, high-lifetime-risk person the ten-year number waves through. Under the new rule, an adult aged 30 to 59 whose thirty-year risk crosses 10 percent can reasonably be started on a statin now, even when the ten-year number looks harmless. One analysis put the potential expansion near 20 million more Americans, concentrated in the younger and middle-aged groups this study found untreated. It is not a new drug. It is the same cheap generic, offered earlier, on purpose.
The second group is anyone the system reaches less well. In US data, statin use runs around 38 percent in white adults and closer to 24 percent in Black and Hispanic adults, a gap that survives even after you account for how sick people are. Blood pressure control follows the same lines, lower in Black and Hispanic patients and far lower in people without insurance, where only about 31 percent have it under control against 53 percent of the insured. The people most likely to be on these drugs, and to have their numbers under control, are older, insured, and white. If you are not in that group, the national average is not describing you.
Two numbers are not the whole body
I want to be honest about what this study does not say, because the easy misinterpretation is dangerous. Bringing blood pressure and cholesterol down is genuine harm reduction. It is not a cure for obesity, and it touches only two of the problems.
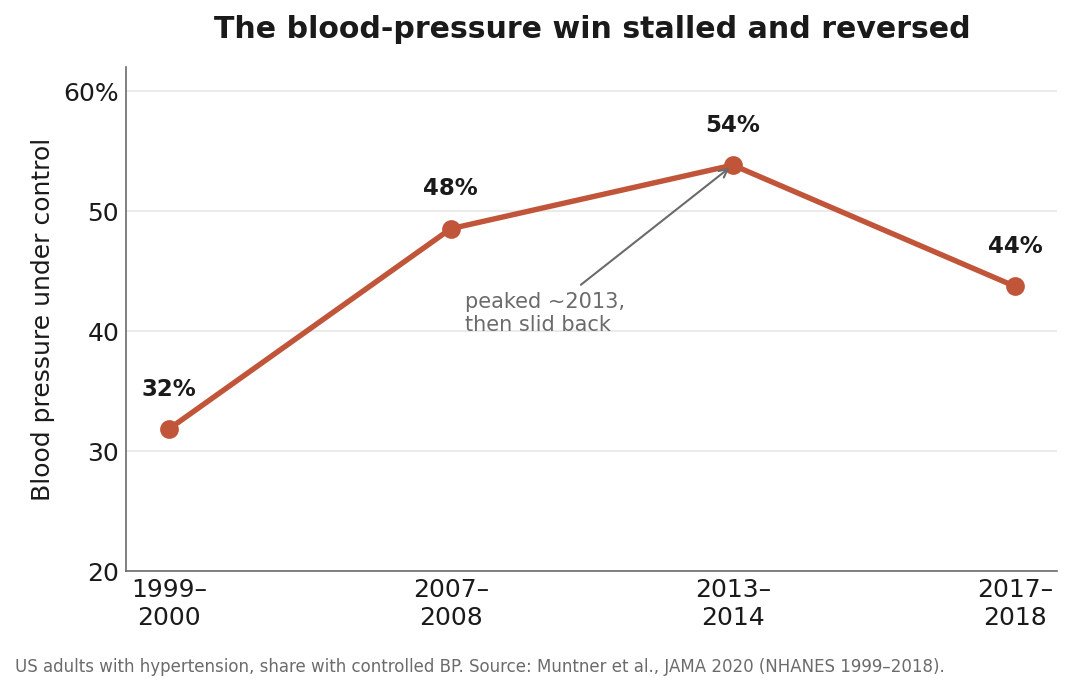
Statins and blood pressure pills do nothing for diabetes, fatty liver, the strain on your kidneys and joints, sleep apnea, or the dozen-plus cancers tied to excess weight. And the heart story itself is not a clean victory either. US blood pressure control climbed through the 2000s, peaked near 54 percent around 2013, and then slid back to about 44 percent by 2018. We are not simply getting better every year.
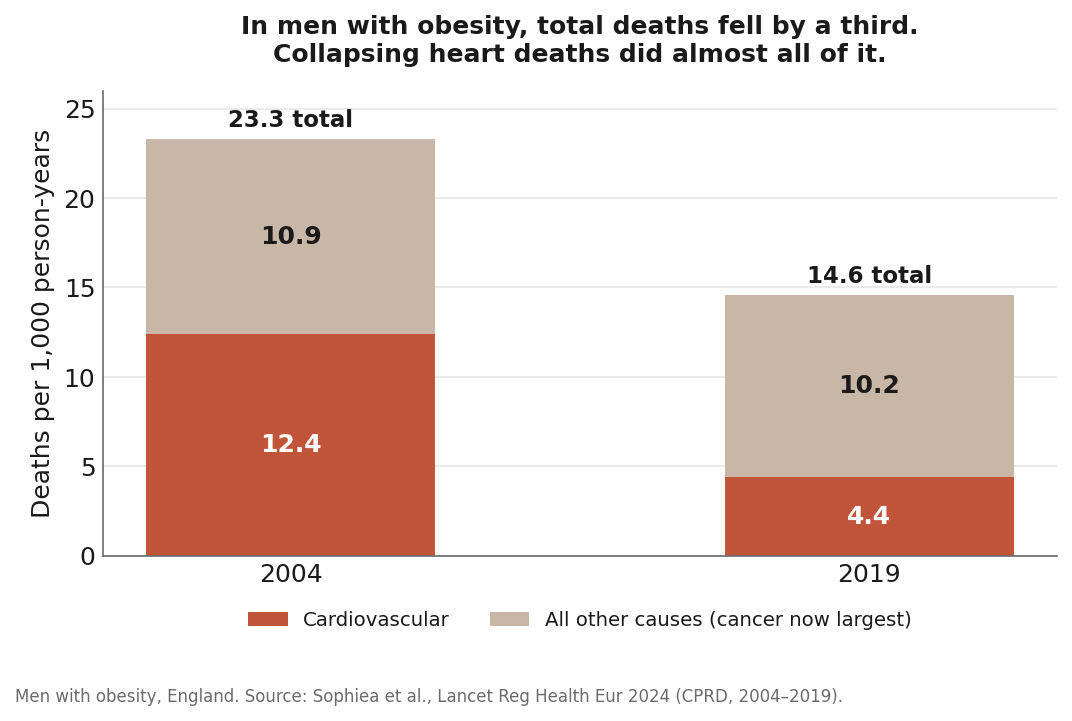
England has the clearest data on where this leads. Researchers there followed mortality by weight from 2004 to 2019. Among men with obesity, deaths from cardiovascular disease were cut by more than half, from 12.4 to 4.4 per 1,000 person-years. But total deaths fell far less, because as heart disease receded, cancer moved up to rival it as the leading cause of death in that group. The heart risk came down. The rest did not.
So we got good, cheaply, at protecting the obese heart. We have not made obesity safe. As heart deaths fall, the other risks of carrying extra weight, cancer chief among them, become the larger share of what is left.
None of this is an argument against the newer drugs. If you are on a GLP-1 like I am, or thinking about one, they have their own heart data now, and it is good. In people with obesity and existing heart disease, semaglutide cut the rate of heart attacks, strokes, and cardiovascular deaths in a large trial. The point is narrower. This particular thirty-year improvement mostly happened before those drugs arrived, on medicines that cost a few dollars a month.
So the practical read, for me, is to stop letting the scale be the only number in the room. After 50, your blood pressure, your non-HDL cholesterol or ApoB, your A1c, your waist, your sleep, and your kidney markers each tell a different part of the story. A GLP-1 may move some of them. A generic you already take may be quietly handling others. The mistake is assuming any one tool covers the whole map.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, and prostate or cancer screening.