
Most “AI predicts disease” papers don’t survive a second read. This one does, and it points at a kind of heart risk your echo was never built to see.
I’ve spent my whole career in machine learning, so I read the steady drip of “AI predicts your death” headlines the way a mechanic reads ads for miracle fuel additives. Most of them are the same trick underneath. Pour a pile of patient data into a neural network, let it find correlations, and call the result a breakthrough. Usually the model learned something boring or fragile, like which hospital took the scan, and it falls apart the moment it meets data from anywhere else.
A paper published in Nature this week did several things these papers usually fail to do, and the thing it found should matter to anyone who has ever walked out of a cardiologist’s office holding a normal test result and a vague sense of relief. Up front, so the rest reads honestly: you cannot get this test, and it has not been shown to save anyone yet. I still think it is worth understanding, and here is why.
A team led by Ziad Obermeyer, a physician and researcher at the University of California, Berkeley, trained a model on hundreds of thousands of electrocardiograms, the cheap electrical heart tracing you have probably had a dozen times. The tracings came from an entire region of Sweden, linked to records of who later died suddenly, meaning an out-of-hospital death from a cardiac cause in the year after the ECG.
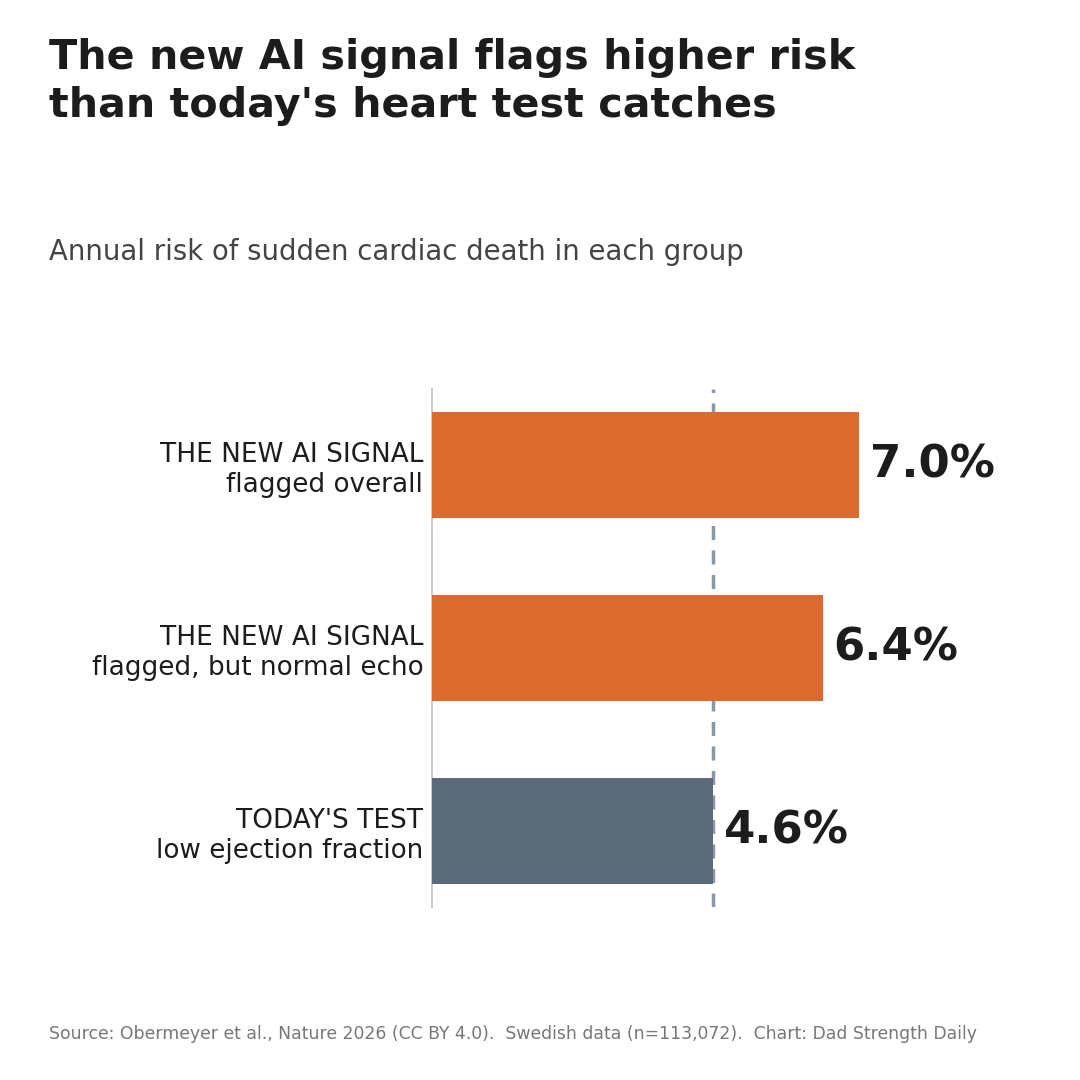
In a held-out test of 113,000 of those tracings, the model flagged a small group, about 2 percent of patients, whose risk of sudden cardiac death over the next year ran around 7 percent. The background rate in everyone else was about half a percent. So it was pointing at people at more than ten times the usual risk of dropping dead, from a test that costs about as much as lunch.
The honest flip side is that more than nine in ten of the people it flagged will not die in the year ahead, and no treatment has yet been proven to help them. This is a sharper way to find risk, not a death sentence and not a reason to start implanting devices.
The one number that decides who gets a defibrillator
What matters is who those people were. Today, when a doctor wants to know whether you are at risk of dropping dead from a sudden heart-rhythm collapse, the call on a preventive defibrillator still leans heavily on one number: the ejection fraction, the share of blood your heart’s main chamber pushes out with each beat, measured on an ultrasound. Below about 35 percent, you become a candidate for an implanted defibrillator, a device that can shock a lethal rhythm back to normal. Above it, you are usually told your heart function looks fine.
The uncomfortable thing cardiologists have known for years is that this number misses most of the people who actually die. In one Oregon study of sudden-death victims, only about a third had an ejection fraction low enough to have ever qualified for a defibrillator. The rest had hearts that pumped normally right up until the day they didn’t. For more than half of the men sudden arrest kills, it is the first sign of any heart trouble at all. The one measurement we hang the whole decision on was never built to catch the bulk of the problem.
That is the gap this model walked into. Of the high-risk patients it flagged, 86 percent would not have been caught by the ejection-fraction test. Even among people whose heart function measured completely normal, the model pulled out a group at higher risk than the patients we currently implant defibrillators in. It is not rediscovering the people we already worry about. It is finding a population that is invisible to the ejection-fraction test we rely on.
Why I didn’t dismiss this one
I take this one more seriously than most, and the reasons are specific.
They locked away 40 percent of their data before they ran a single analysis and didn’t open it until the journal had already agreed to publish, so there was no way to quietly tune the model until it looked good and then call that a result. When they finally ran the finished model against that sealed data, once, it held up. That discipline is rarer than it should be. Tuning a model against your own test set until it sparkles, then presenting the sparkle, is the most common way this kind of study fools everyone, including the people who built it.
They also checked whether the finding traveled. A pattern learned in Sweden could easily be Swedish noise, so they ran the same model, untouched, on hospital data from the United States and from Taiwan, recorded on different brands of machine. It still worked. They even ran a sanity check I liked: the model was sharp at spotting the rhythm-driven deaths it was built to catch, and close to useless at flagging deaths from other causes like lung or brain failure. That is exactly what you want to see, because it means the model locked onto something specific to the electrical fault, not a vague signal that someone is sick.
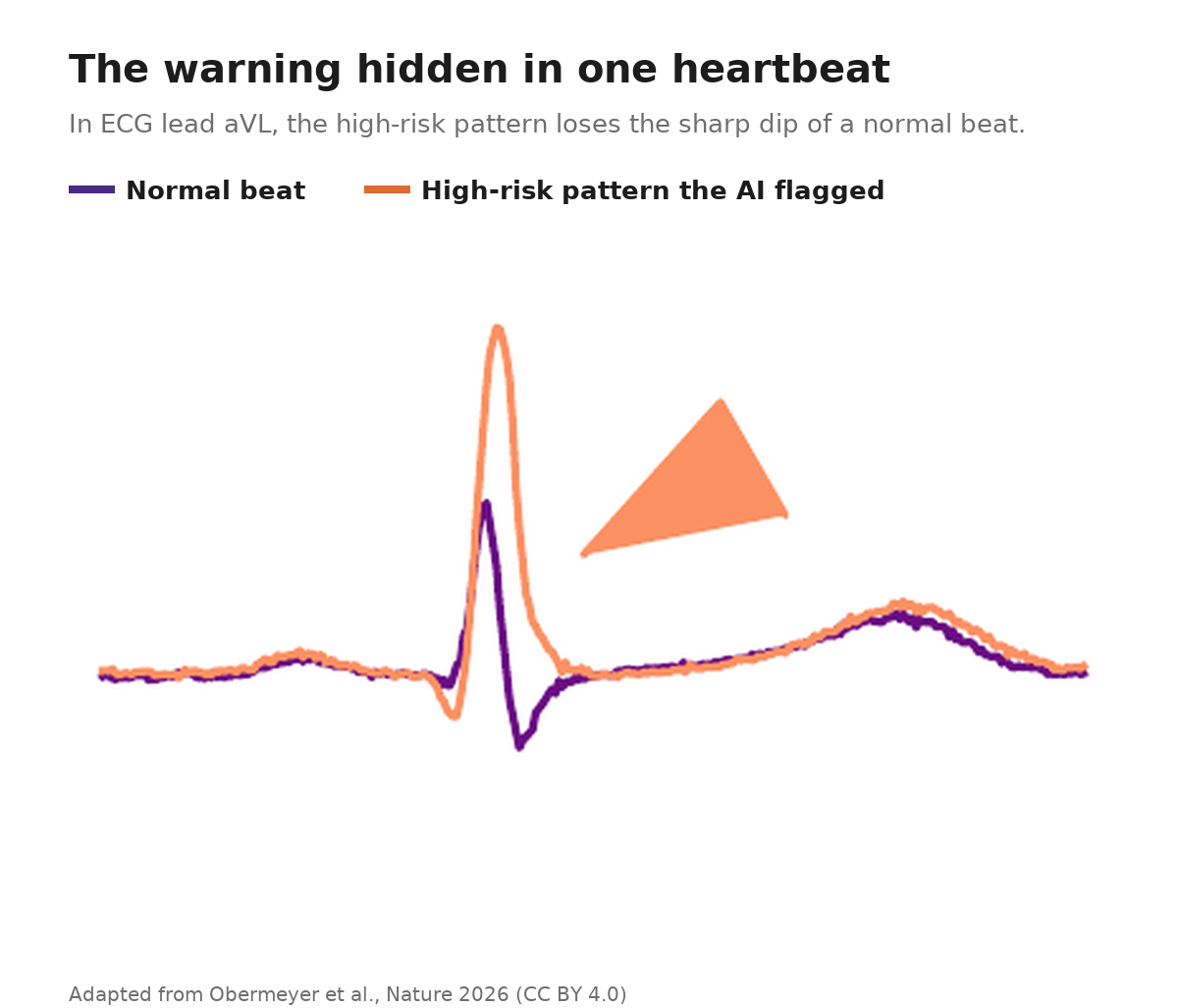
What got me, though, is that they didn’t stop at “the model works.” They tried to figure out what it was seeing. A model that spits out a risk score is a fortune teller, so they built a second model that could draw realistic ECGs and used it to morph a low-risk tracing into a high-risk one, step by step, until they could see what changed. What changed was a specific, never-before-described squiggle in one lead, called aVL, which is just one of the twelve angles an ECG views the heart from. The sharp downstroke of a normal beat softened into a slurred little tail.
When they went looking for what could produce that shape, it traced back to diffuse scarring spread through the heart muscle, a known setup for fatal rhythms. Here is the detail I keep coming back to. For the high-risk patients who happened to have a heart MRI on file, a blinded re-read found that scarring sitting right there, even though it had not surfaced in the clinical notes after those scans. In fairness to the cardiologists, this kind of diffuse, spread-out scarring is genuinely hard to see unless you already know to look for it. That is sort of the point. The cheap tracing seemed to know where to look.
That is where I stopped thinking nice prediction trick. The model didn’t just rank people, it pointed at a mechanism researchers can now go test: a visible feature on the ECG, pointing at possible diffuse scar, pointing at the electrical instability that sets off sudden death.
Why you can’t buy this yet
You cannot get this test. It is not approved or sold, and your doctor cannot order it. It is a research finding.
It also has not been shown to save a single life yet. Knowing who is at risk is not the same as proving a defibrillator helps them, and the history of this field is full of promising risk markers that flagged “high-risk” people who turned out not to benefit. That matters more than it sounds, because the device is no free lunch. Defibrillators bring infections, lead problems, and inappropriate shocks, and most never deliver a life-saving shock. The authors say all of this plainly and call for a proper randomized trial. And while the prediction held up in the sealed test, the discovery half, the scarring story, was worked out on the looser part of the data and is best read as a strong lead, not a settled fact.
Outside experts are cautious too. Sumeet Chugh, the Cedars-Sinai electrophysiologist whose Oregon research showed how badly ejection fraction misses, told STAT the tool might one day help sort risk, but “it’s a long road to even getting close to the patient.” The team is trying to shorten it. They have a follow-up study underway that links the ECG predictions to actual heart-muscle biopsies, to pin down the scar connection, and Obermeyer points out that wearable defibrillator patches could make a real trial practical. “You might not want to go get surgery right away,” he said, “but you could be persuaded to wear a patch for a few months just in case.”
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
What I’d actually do with this
So what do you do with this today, as a man somewhere around fifty who would prefer not to die suddenly?
Mostly, you update one belief. A normal echo is not a clean bill of electrical health. It answers one narrow question about how hard your heart squeezes, and the thing that kills most people who die this way lives outside that question. About 4 in 10 of the sudden-death victims in this study had no obvious risk factor flagged at the time of their ECG.
A couple of things not to do first. Don’t go hunting for an AI-ECG app, and don’t read one paper as a reason to ask for a defibrillator. Neither is earned yet. What you can act on is the unglamorous stuff that actually moves risk. Know your blood pressure and your ApoB, the count of cholesterol-carrying particles that drive heart disease, the way you know your weight. Get unexplained fainting or a racing heart looked at instead of shrugging it off. Find out whether anyone in your family died suddenly and young. Those are the levers that exist right now.
None of this is medical advice, and I am not a doctor. If your own numbers or symptoms have you worried, that is a conversation for your doctor, not a blog post.
I find this genuinely hopeful, and not because there is anything to buy. For years, the honest answer to “who is the healthy-looking guy about to die of this” was a shrug. I am not changing what I do tomorrow. But this is the first real step I have seen toward a better answer than a shrug, and I am watching it closely.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.