
Testosterone would get an Olympian banned. The GLP-1, not yet. I take both, and here is what they actually did for a normal fifty-year-old body.

I take two drugs that sit at the heart of sport’s fight over what counts as cheating. One of them, testosterone, would get an elite athlete banned tomorrow. The other, the GLP-1 tirzepatide, in the same family as Ozempic and Wegovy, nobody has banned yet. I am not an athlete and I never will be. I am a man in his fifties with a bad knee and a garage gym, and between them those two drugs handed me back a body that works.
The word “doping” has been trailing GLP-1s around all month. Serena Williams returned to professional tennis at 44, and she has been open that a GLP-1 helped her drop 34 pounds and get back into playing shape. She is a paid spokesperson for the telehealth company Ro, she is, as The Atlantic put it, the first active elite athlete to publicize using one, and the tennis world immediately started asking whether that counts as cheating, as Nicholas Florko laid it out. The World Anti-Doping Agency is watching. For now, athletes are free to take them.
I read that whole argument from the other side of the glass. The rules that decide whether Serena is “enhanced” have nothing to do with me. I am not chasing a ranking. The only thing these drugs enhance in my life is my ability to climb a flight of stairs without planning for it, and to put a loaded barbell on my back at an age when most men my age are quietly giving that up. Call it legal doping for the rest of us. Both are prescribed and monitored. The point here is what they made possible, not what anyone else should copy.
What a sedentary man’s body does after fifty if he does nothing
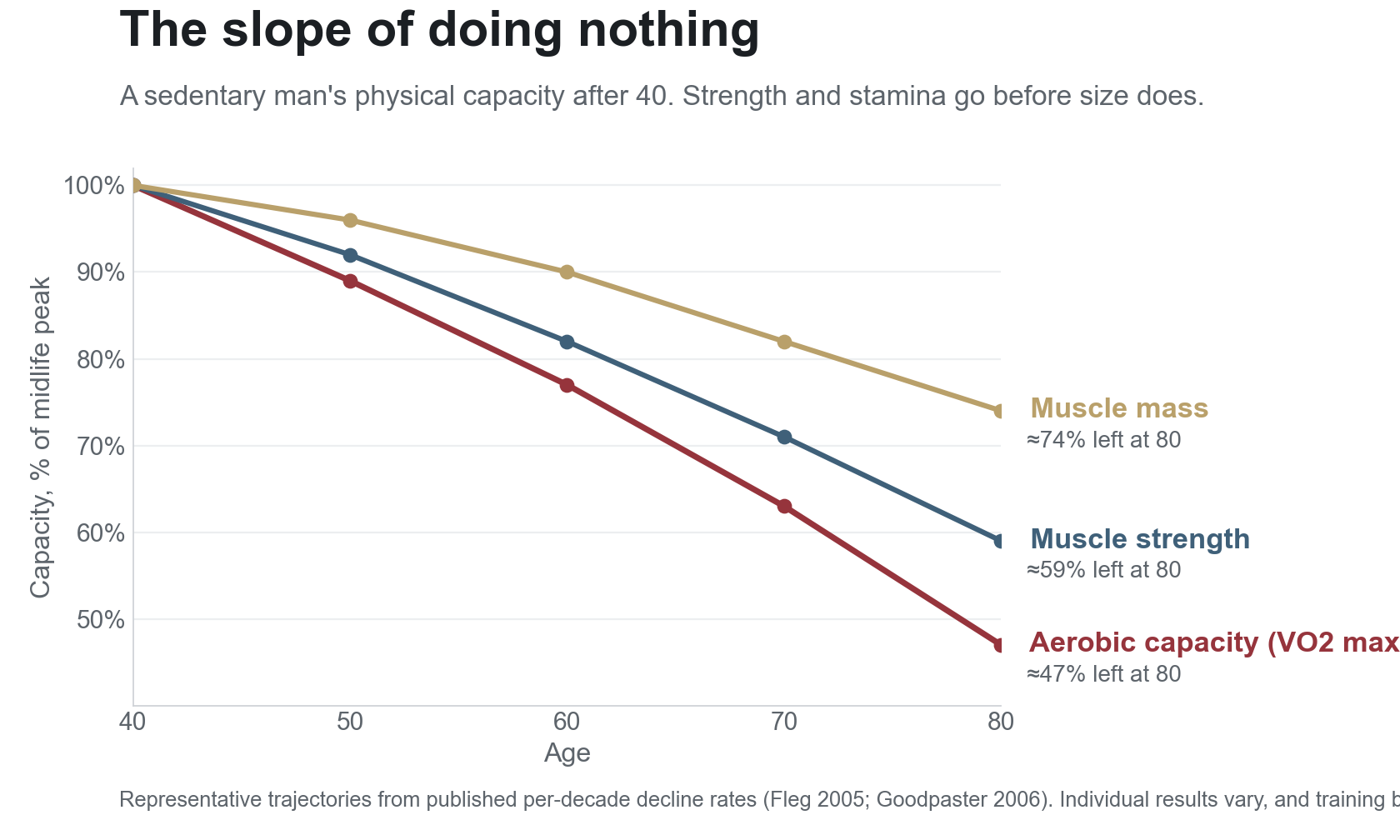
The opponent is not Father Time in some soft, greeting-card sense. It is a measurable slide, and it is steep.
The muscle is the first thing to watch, and here is the part most men miss: strength fades about three times faster than size, so you lose the ability to do things well before the mirror tells you anything is wrong (Goodpaster, Journals of Gerontology, 2006). Aerobic capacity, the engine behind walking up a hill without stopping, drops roughly 10% per decade and speeds up after 50 (Fleg, Circulation, 2005). Testosterone drifts down with age too, but less than the “low T epidemic” ads imply, and it falls more with weight gain and poor health than with age alone (Wu, New England Journal of Medicine, 2010).
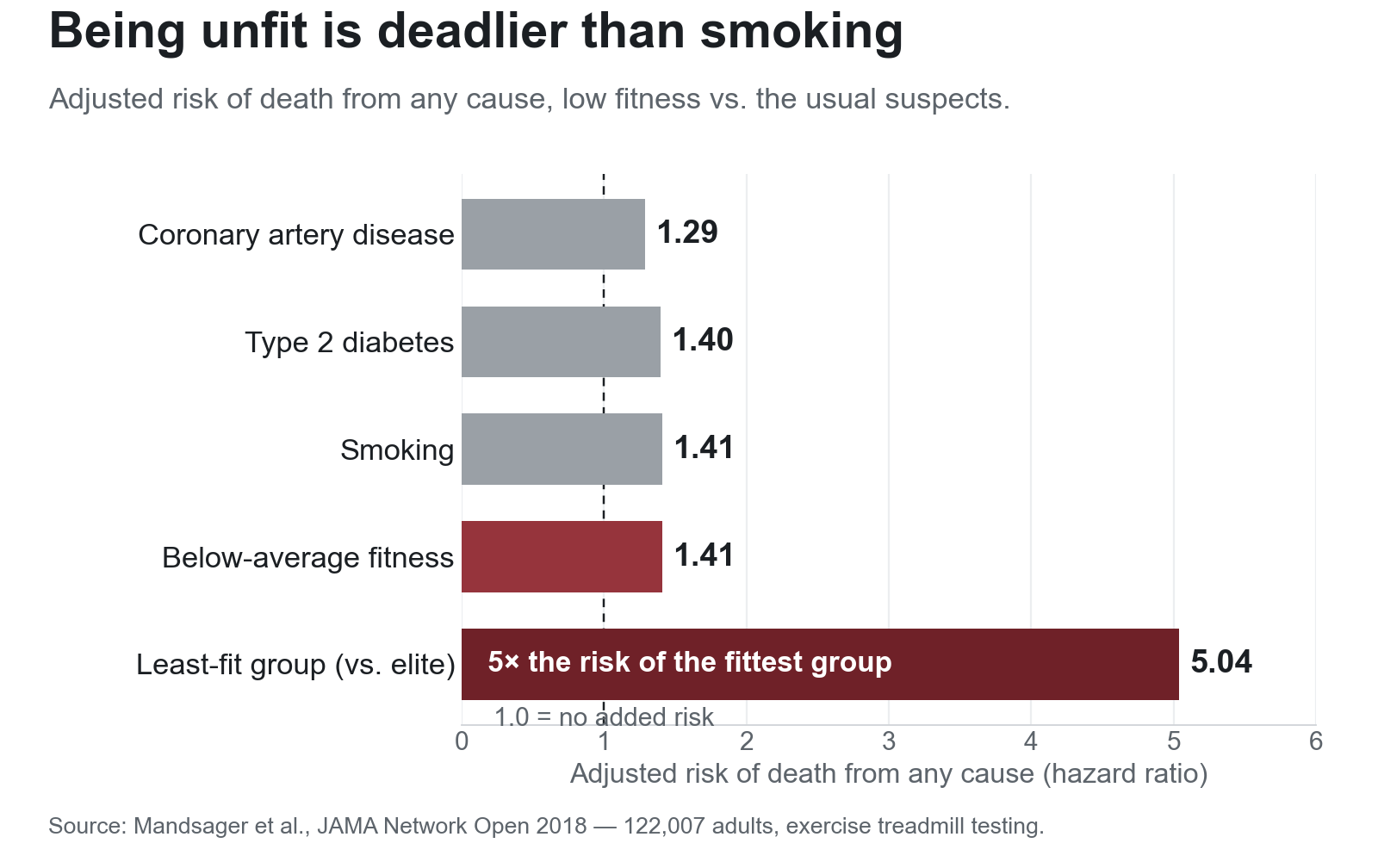
None of that is the scary number. This is the scary number. In a study of 122,007 people, the least fit group had a death rate five times the fittest group, and being unfit carried a mortality risk equal to or worse than smoking, diabetes, or established heart disease (Mandsager, JAMA Network Open, 2018). Low fitness is not a vanity problem. In the mortality data, it shows up on the same scale as a pack-a-day habit.
And almost nobody is doing the one thing that fixes it. When researchers strapped activity monitors on adults instead of asking them to self-report, fewer than 5% actually hit the basic guideline of 150 minutes of moderate activity a week (Troiano, Medicine & Science in Sports & Exercise, 2008). That is the default setting for a man at 50 who changes nothing. Less testosterone, less muscle, less air in the tank, less movement, each one feeding the next.
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
Testosterone has been banned in sport since the 1970s, and my dose is 120 milligrams a week
The doping angle is not just a headline to me. Testosterone is the original performance-enhancing drug. It was first made in the 1930s and was building Olympic weightlifters by the 1950s, and it sits on the WADA prohibited list today under Class S1, banned in competition and out of it, all year round. An athlete with genuinely low levels can apply for an exemption, but the bar is high enough that ordinary age-related or weight-driven decline does not clear it.
My dose is 120 milligrams a week. Before it, my total testosterone read 181, under the floor of the normal range; replacement brought it back into normal territory, and I get my blood count and prostate marker checked on a schedule to keep it safe. That is replacement, not a cycle, and my case, not a template for yours. People hear “testosterone” and picture a guy with a 20-inch neck. That is not this. In the study that defined what testosterone can do, Shalender Bhasin gave healthy men 600 milligrams a week, five times a replacement dose, and they gained roughly 13 pounds of lean mass in ten weeks without lifting a thing (New England Journal of Medicine, 1996). That is the doping dose. That is not what a man on TRT is doing, and any honest version of this story has to say so out loud.
I know more than a few guys running the serious stuff, the bodybuilding doses, and I find that world genuinely fascinating: the diet, the training, the “supplementation” nobody prints on a label. I have no interest in going there myself, for health reasons and legal ones both. A replacement dose keeps me where a doctor will sign the script, and that is the line I want to stay on.
A replacement dose delivers less than the internet promises and more than the doubters allow: in the most careful trial we have, a year of it gave older men with clearly low levels modest but real gains in energy, mood, sexual function, and strength (Snyder, New England Journal of Medicine, 2016). The regulators are catching up. In June 2026 the FDA, citing TRAVERSE, asked drugmakers to drop the old label line that called testosterone’s benefit in age-related low T “not established” (HHS). For me it was never magic, just the hormonal headwind lifting so the work finally showed up. Before TRT, training felt like pushing a car; after, the same work moved me.
The GLP-1 didn’t just shrink me, it let me move again
The testosterone gave me back recovery and drive. The GLP-1 gave me back the ground under my feet, by taking weight off it.
The weight-loss part is not the mystery. On semaglutide, people lost about 15% of their body weight over a little more than a year (Wilding, New England Journal of Medicine, 2021), and tirzepatide, what I take, runs higher than that. I lost about 170 pounds getting here, a lot of it on tirzepatide, and that is its own long story (told in full here). The number I care about now is not on the scale, though. It is what dropping the weight let me do. The trials show the same thing: people carrying extra weight and living with heart failure did not just shrink on these drugs, they felt better and walked farther (Kosiborod, New England Journal of Medicine, 2023). My knee stopped screaming, and the workout that used to feel impossible became a normal day.
The catch is the muscle. A chunk of any large weight loss is lean tissue (including muscle), not just fat, which is why I will not stop nagging about protein and the gym. Across the trials, somewhere between a quarter and 40% of the weight people lose on these drugs is lean mass (Sargeant, Endocrinology and Metabolism, 2019); a 2026 analysis of seven trials put the average lean-mass loss around 1.74 kilograms, though as a share of a now-smaller body, lean mass actually rises (Laverde, International Journal of Obesity, 2026). Sit on the couch through that and you become a smaller, weaker version of yourself. Lift through it with enough protein and most of what you lose is fat, not muscle. The drug does not decide which one happens. You do.
The drugs give you the floor, lifting heavy things builds the rest
Both the hype and the sneering miss the same thing: these drugs are not a shortcut to fit & strong. At a replacement dose, testosterone only restores a level I used to have on my own; the GLP-1 only cleared the weight and the appetite that kept me parked. Neither one does a single rep for you.
For most of my forties I was 170 pounds heavier than I am now, and I could talk myself out of any workout before it started, not because I was lazy but because my body could not answer the effort. The drugs fixed that part. The change itself happened in my garage gym, five days a week, on a program my coach writes, on the bike when my knee says no.
What it costs, and who should be careful
None of this is free.
Testosterone’s cardiac reputation, for years the big fear, mostly held up to scrutiny: in a trial of more than 5,000 men at high cardiovascular risk, TRT did not cause more heart attacks than placebo (Lincoff, New England Journal of Medicine, 2023). But the same trial flagged more atrial fibrillation, more blood clots, and, in a follow-up, more broken bones, most of them from ordinary falls, for reasons nobody has fully explained (New England Journal of Medicine, 2024). It also thickens the blood and shuts down your own production. That mixed picture is exactly why I get bloodwork on a schedule and why a real doctor, not a “wellness clinic” with a sales quota, manages this. GLP-1s carry their own short list: nausea, gallbladder trouble, and muscle loss if you skip the protein and the lifting. These are tools with edges. Use them with a doctor and your eyes open.
None of that scares me off the trade. We have spent a decade arguing about whether athletes who use these drugs are cheating, and almost nobody asks the more useful question: what they do for the millions of ordinary men sliding down the curve I started with. They hand a tired, heavy body back its opportunity, and that opportunity is the part most of us were missing. At 50-plus, with weights in the garage and a body that finally answers, the work is worth doing again.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.