
He goes to AA every week and recently started the Wegovy pill, hoping it quiets what’s left. Here is what ninety years of alcohol treatment, from the Twelve Steps to a weight-loss drug, actually shows.
I have a buddy from college who has been sober for years. He does everything the program asks. He goes to a meeting most weeks, he has a sponsor, he has the chips that mark the time. And he still gets the cravings. Not the dramatic, white-knuckle-on-the-bar kind you see in movies. The quieter kind. A low background hum that never fully switches off, the part of the brain that keeps raising the subject of a drink long after the rest of him has moved on. People who take GLP-1 medications for their weight have a phrase for the food version of this. They call it food noise. My buddy has the drinking version, and a month ago he started the Wegovy pill, the oral form of semaglutide, hoping it might turn the volume down.
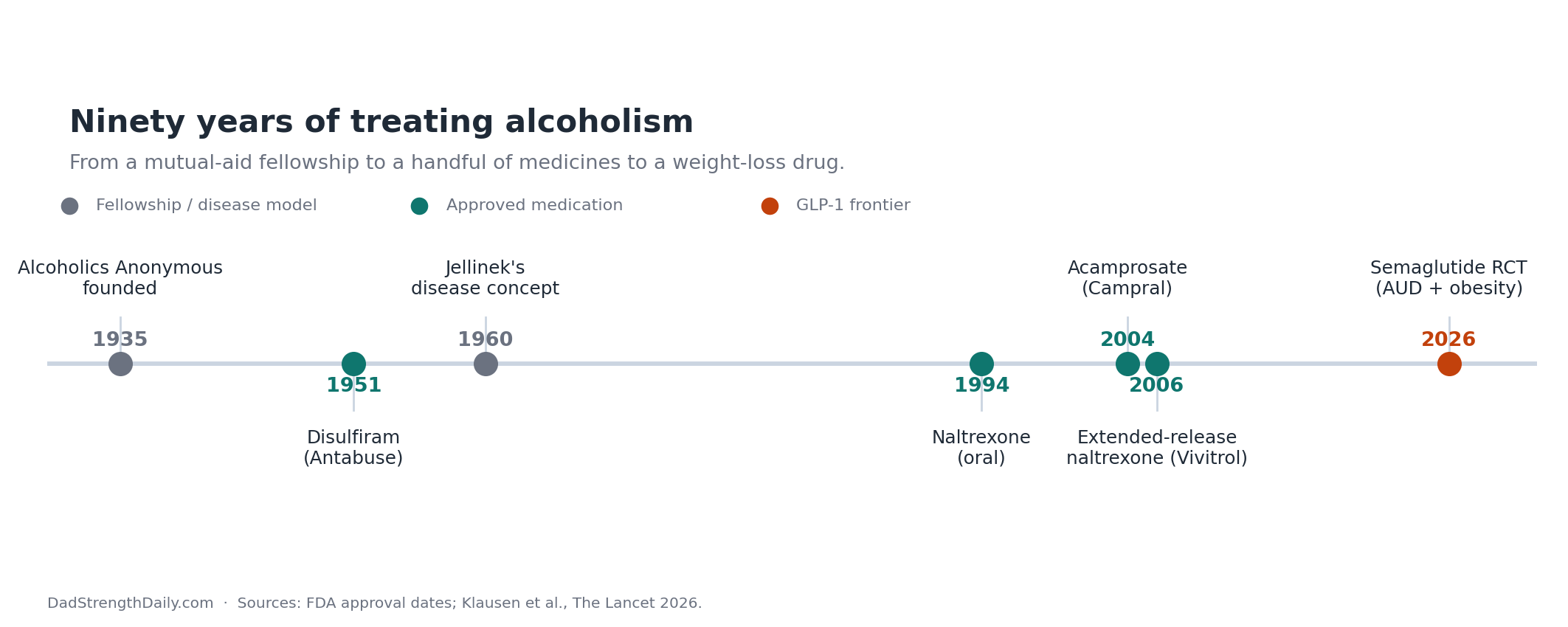
I keep turning that hope over. I quit drinking in my own forties, but I never had cravings for a drink, and I have spent a good part of this year reading about why some people get free of it and some people carry it for decades. The short answer is humbling. We have been trying to treat this for about ninety years. It built one of the most famous self-help movements in history and we developed a small set of genuinely useful medicines along the way. And we still cannot reliably switch off the circuit that wants the drink. So when reports and early studies began to suggest that a diabetes shot might quiet cravings as a side effect, people in recovery paid attention. My buddy paid attention.
So I read the way the question demanded, across the meetings, the medicines almost no one is offered, and the new drugs aimed at the craving itself. This is the version I wish I could have handed him over coffee, instead of the half-answers I managed at the time.
The fellowship that built American recovery
Two men founded Alcoholics Anonymous in 1935, a stockbroker named Bill Wilson and a surgeon named Bob Smith, both of them drinking themselves toward early graves until they got sober by leaning on each other and on a Christian fellowship called the Oxford Group. Out of that came the Twelve Steps: admit you are powerless over alcohol, turn it over to a higher power, take a moral inventory, help the next person who is still sick. It spread faster than any recovery movement before it.
By the 1950s, the idea underneath it had hardened into something close to medical doctrine. In 1960 the physiologist E.M. Jellinek published *The Disease Concept of Alcoholism*, which reframed the heavy drinker as a patient rather than a sinner. That reframing did real good. It pulled alcoholism partway out of the moral gutter it had sat in since the temperance era. It also fused with AA to produce the Minnesota Model, the blueprint for the classic twenty-eight-day rehab, and for decades that combination was simply what treatment in America meant. Courts ordered people to meetings. Employers did too.
AA’s strongest defenders and its sharpest critics tend to skip the same inconvenient fact. Because the fellowship is anonymous, decentralized, and at least partly spiritual, it spent most of its life impossible to study properly. The skeptics had a real point: people who stick with any program are more motivated than the ones who quit it, so AA’s success stories might just be the motivated people selecting themselves. Nobody could cleanly separate the program from the kind of person it attracts.
Then the researchers found a way in. They tested a structured, manual-based version of twelve-step work that a clinician delivers, which can be randomized the way a drug can. The biggest verdict came in a 2020 Cochrane review that pooled twenty-seven studies and more than ten thousand people. It found that this manualized twelve-step approach produced higher rates of continuous abstinence than other respected talk therapies like cognitive behavioral therapy, and did it at lower cost. The likely active ingredient turned out not to be the higher power at all. It was the network. AA works by rebuilding your social world around people who are not drinking, by handing you coping skills, and by slowly convincing you that you can actually do this.
My buddy is the living proof of both halves of that finding. The meetings are the thing holding the line. They are also not enough to silence the craving, and the program’s one-size answer, total abstinence or nothing, gives him no language for the part that is still loud. AA got him sober. It did not get him quiet.
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
The medicines almost no one is offered
While the fellowship owned the culture, a quieter track was developing in pharmacology, aimed at the biology underneath the habit. The strange thing is how little of it ever reaches the people who could use it.
The first drug, disulfiram, arrived in 1951 under the name Antabuse. It does not touch craving at all. It makes you violently ill if you drink, the chemical equivalent of a tripwire, and the catch is that it only works when someone you trust watches you take it. Left to take it on our own, most of us simply stop on the days we want to drink. It is rarely a first choice now.
The real shift came in 1994 with naltrexone, a pill that blocks the opioid receptors alcohol leans on for its glow. Take away the glow and, for a lot of people, the second and third drink lose their pull. The best summary we have, a 2014 review in JAMA that pooled fifty-three trials, put numbers on it. Treat about a dozen people with naltrexone and one of them who would have gone back to heavy drinking does not. Modest, but real, and better than most of what medicine offers for a chronic relapsing condition. Most people who are prescribed it take it as a daily pill, drinking or not, to lower the risk of relapse and heavy drinking over time. A Finnish researcher named David Sinclair built a method around a different schedule, the idea that you take the pill an hour before you plan to drink, so that drinking with the reward switched off gradually unlearns the habit itself. He called it pharmacological extinction. It has a devoted following and a logic that fits how the brain actually learns. Notice, though, what naltrexone is built for: it dulls the payoff when you do drink. For someone who is already not drinking, the craving that shows up between meetings is a different target, which is part of why the newer drugs caught people’s attention.
A few more followed. Acamprosate, approved in 2004, eases the long, grinding restlessness that lingers for months after the last drink and pulls people back. It works well in European trials and oddly poorly in American ones, and the big U.S. COMBINE trial in 2006 found no benefit from it at all, while naltrexone held up. Then came the version of naltrexone my buddy has never been offered: Vivitrol, a once-monthly injection approved in 2006 for people who cannot keep a daily pill going. Its pivotal trial cut heavy drinking days by about a quarter against placebo. Off to the side sit a handful of repurposed neurology drugs, topiramate and gabapentin among them, with weaker but genuine evidence.
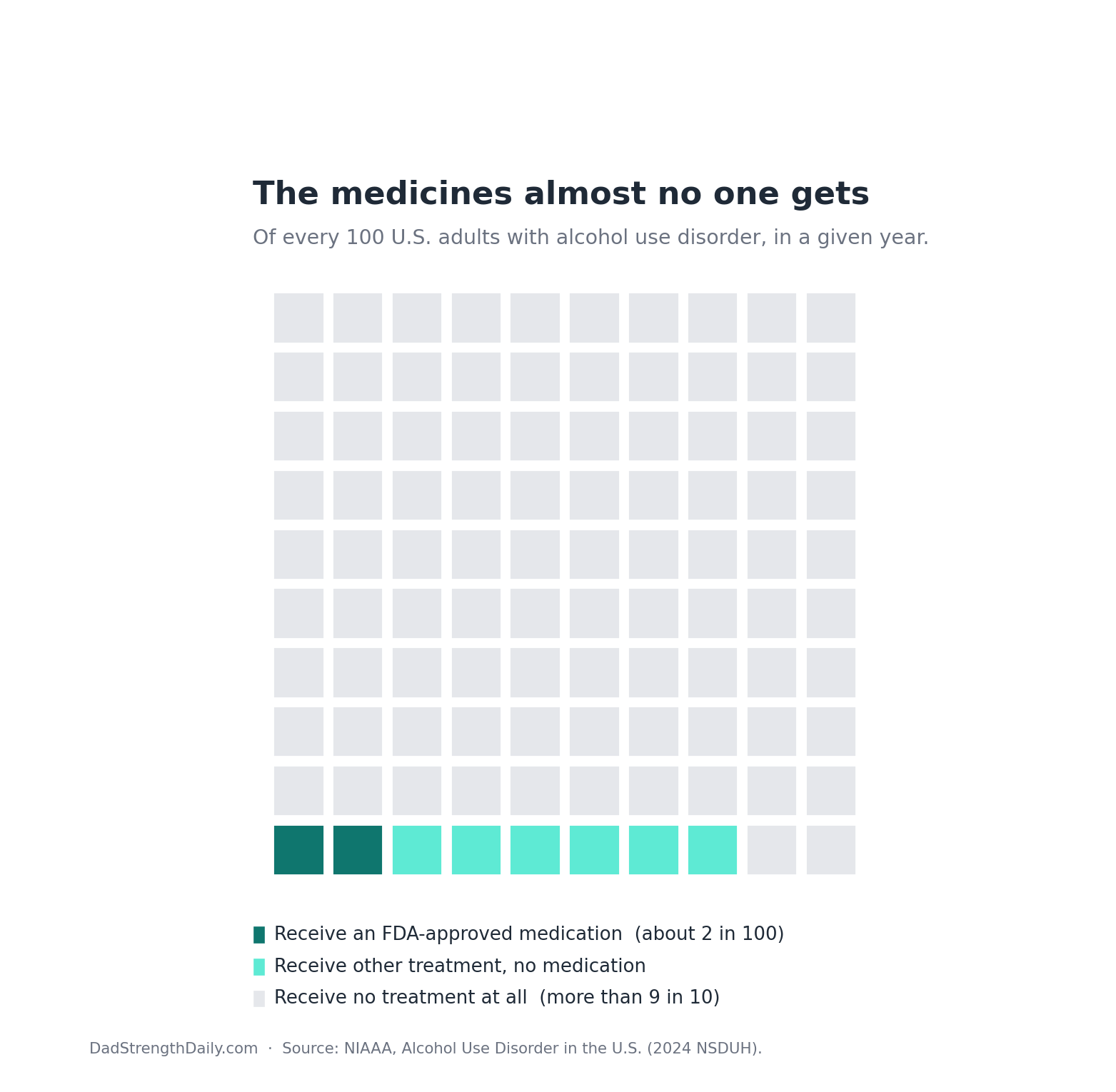
So we have a menu. Now the number that should bother you: only about two percent of people with alcohol use disorder get one of these medications in a year, even though the American Psychiatric Association and the VA recommend them. Count every kind of help, and fewer than eight in a hundred get any treatment at all. The reasons are cultural more than scientific. Addiction care grew up walled off from regular medicine, so the doctor you actually see rarely prescribes it. And the abstinence culture that AA built carries a quiet suspicion that a pill is just trading one drug for another. My buddy has spent years doing the hardest version of this, the meetings and the inventory and the honesty, and as far as I know no one ever mentioned that there was a prescription that might take the edge off. That gap, between what works and what gets used, is the real scandal sitting inside the success story.
If you are the one doing the meetings and still fighting it, here is the practical part. Prescriptions exist for exactly this, and most people never hear about them. It is worth asking your own doctor about naltrexone, acamprosate, or the monthly Vivitrol shot, and whether any of them fit you. That is not medical advice from me, and a GLP-1 for drinking is still off-label. It is a short list to bring to an appointment that usually skips it.
The noise that outlasts the last drink
A craving is not a character flaw, whatever the old temperance preachers thought. It is a circuit. Drinking trains a deep one, the mesolimbic dopamine system, the same wiring that evolved to make food and sex and safety feel worth chasing. Alcohol hijacks it and turns the dial up. Get sober and your behavior changes, but that wiring stays sensitized for a long time, sometimes for good, which is why years of clean time can coexist with a craving that still ambushes you in a grocery-store parking lot. The drinking stops well before the wanting does.
GLP-1 drugs were never meant to go anywhere near this. They were built to manage blood sugar and then, almost by accident, to take weight off, because they slow the stomach and dial down appetite. But GLP-1 receptors also sit in those reward regions of the brain, and the working theory is that the drug there blunts the dopamine spike alcohol produces. I want to be careful with the word theory. Less drinking could also ride on nausea, a smaller appetite, the weight coming off, or just feeling different, unless a study is built to rule those out. One clue that something more specific is going on comes from a 2025 study: drugs that only nudge your own natural GLP-1 upward do nothing for drinking. You seem to need the actual medication reaching the brain, which points to a real drug effect rather than a pure placebo story.
The early signals were hard to ignore. Rats drank less. So did African vervet monkeys, which take to alcohol on their own and are about as far from a motivated AA member as a research subject gets. Then the human data scientists went digging through medical records. The largest analysis, published in 2024 and built from more than eighty thousand patients with obesity, found that people on semaglutide were roughly fifty to fifty-six percent less likely to be newly diagnosed with alcohol use disorder, or to relapse into it, than people on other weight medications. That is an enormous gap, and also exactly the kind of finding that records can only hint at, never prove, because the people who get one drug are never quite the same as the people who get another. One thing to keep clear before going further: none of this is approved for drinking. Every use here is off-label and early.
The trial was real. So were the limits.
The cleaner test, the one that actually randomizes people, took a while, and the first attempt looked like a failure. A 2022 trial of a related drug called exenatide missed its main target. Across the whole group, it did not cut heavy drinking. Buried in the data, though, was a signal that refused to die: in the patients who also carried extra weight, it worked.
Semaglutide itself got its first randomized test in 2025, when a US team gave forty-eight people with alcohol use disorder either a low dose or a placebo for nine weeks (JAMA Psychiatry). It was small, and the results were split: it did not change how many days people drank, but it cut how much they drank on those days, lowered their craving, and bent heavy drinking down over time. The authors called it what it was, early evidence that earned a bigger trial.
That bigger trial came from the Danish group that ran the exenatide study, and it landed in The Lancet in 2026. They took 108 people who had both alcohol use disorder and obesity, gave half of them the injectable form of semaglutide and half a placebo, and gave everyone real behavioral therapy on top. Over twenty-six weeks, the share of heavy drinking days fell by about forty-one percentage points on semaglutide against about twenty-six on placebo, a real and statistically solid gap. Total alcohol intake dropped by roughly a drink a day more than placebo. In plain terms, fewer heavy days and less alcohol overall, though not sobriety. For a larger early trial in this population, that is a striking result, and it is why my buddy’s hope is not foolish.
I’d slow down here, because the fine print matters more than the headline. The drug reduced drinking. It did not produce abstinence, and for someone whose entire program is built on not drinking at all, the difference between less and none is not a footnote. Everyone in the trial also got therapy, so semaglutide was the thing added to the work, not a replacement for it. Every single participant had obesity, which is the population the drug was tested in and the only one we can really speak about. It was one small trial at a single center. And it was funded in part by the foundation tied to the company that makes the drug, which does not make the result wrong but does belong on the label when you are weighing it. These are also not gentle drugs. Nausea and other gut effects are common, they cost money and can be hard to get, and starting and stopping them is its own project.
Now hold my buddy’s actual situation against that. He is taking the Wegovy pill, the oral form. The trial used the shot. We do not yet know that the pill clears the same bar for drinking, and the doses are not interchangeable. A pill trial has since reported, and it missed its primary endpoint at a dose well below the one he takes. My buddy is also not focused on losing weight. None of that makes the hope unreasonable. It makes it a step or two ahead of the proof, which is a different and more honest thing to tell him than either “this will fix it” or “do not bother.”
The science is not standing still. Eli Lilly is running Phase 3 studies of brenipatide, an investigational incretin being studied directly for alcohol use disorder rather than borrowed off-label from obesity care. If it works and gets approved, this stops being off-label improvisation and becomes an actual treatment, the way naltrexone once did. I have written before about how strange and promising that is.
What I actually told my buddy
I keep noticing the same thing across the decades. Every era showed up promising a cure and left behind a tool. The disease idea was supposed to end the shame, and what it actually did was make the whole subject less moralistic while starting a fight about willpower that is still going. AA was supposed to be enough on its own. It built something medicine never could, and it still sends some people home craving. The pills were supposed to be the answer, and instead they help real people while almost nobody gets handed a prescription. The shot is just the latest cure in the latest box. If it runs true to form, it will end up smaller than the press release and more useful than the skeptics want to admit.
I don’t think 2026 hands us an instant cure. It hands us more choices, more of them than we have ever had: the meetings, the medicines that almost no one is offered, and now a class of drugs that may reach one part of the wiring behind the craving. My buddy is not picking one over the others. He is keeping the years and the sponsor and the weekly chair, and adding a pill on top, betting that the thing which quiets food noise might quiet the other kind too. The evidence says that bet is reasonable and unproven in his exact case, which is the most truthful sentence I can offer him.
A month in, he tells me the noise has dropped, and so has something I hadn’t thought to ask about. Before the pill, he had traded the drink for two or three bottles of sugary root beer a night, a habit he hated and couldn’t put down. Since starting Wegovy, the root-beer cravings are simply gone, and he says the background anxiety has eased a little too. One person, one month, is not evidence, it’s an anecdote. But it matches what the drug seems to do: it doesn’t just quiet the wanting for alcohol, it turns down the reward chase itself, which is why the same trials that lowered drinking also nudged down cigarettes. For someone who spent recovery swapping one craving for another, that’s the part worth watching.
Either way, I told him to keep the meetings. The thing that got him sober is the thing he already built.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.