
The drugs were ordinary. The result wasn’t: a 27-point blood-pressure drop in men medicine usually fails to reach.
A colleague mentioned this interesting hypertension treatment project to me almost in passing, so I looked up the study. A group in Los Angeles turned Black barbershops into blood pressure clinics. Men came in for haircuts and, over several visits with a pharmacist who set up between the chairs, got their blood pressure under control and kept it there for at least a year. It’s the kind of plain, low-tech project that actually reaches the people medicine usually misses, and it’s exactly the kind that struggles to get funded.
What got me wasn’t only that it worked. It was who it worked for. These were men doing the same thing I’d done for most of my adult life, which is ignore my blood pressure until something finally forces the issue.
The number I avoided
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
My mother had high blood pressure her whole life. That’s the kind of family history you’re supposed to act on. I didn’t, for years. I knew the number was sitting in my chart somewhere, the way you know there’s a noise in the car you’ll deal with eventually. I was busy with other things and telling myself the rest would follow. Mostly it did. The blood pressure didn’t get my attention until I finally bought a cuff, started measuring at home, and went on telmisartan to bring it down.
Here’s the embarrassing part. I read studies for a living now. I’ve got insurance, a regular doctor, no real reason to have waited. I waited anyway. If it’s that easy for a guy like me to drift, picture how it goes for a man with no doctor at all, who’s been burned by medicine before and has every reason to keep his distance.
That’s the man this study was built for. I drifted out of privilege. I could’ve walked into any clinic on any day. These men were dodging a system that had earned their suspicion. Same blank where the number should be, very different reasons for it. What I liked about the study is that it took that difference seriously instead of just nagging people to do better.
Not advice. Treatment.
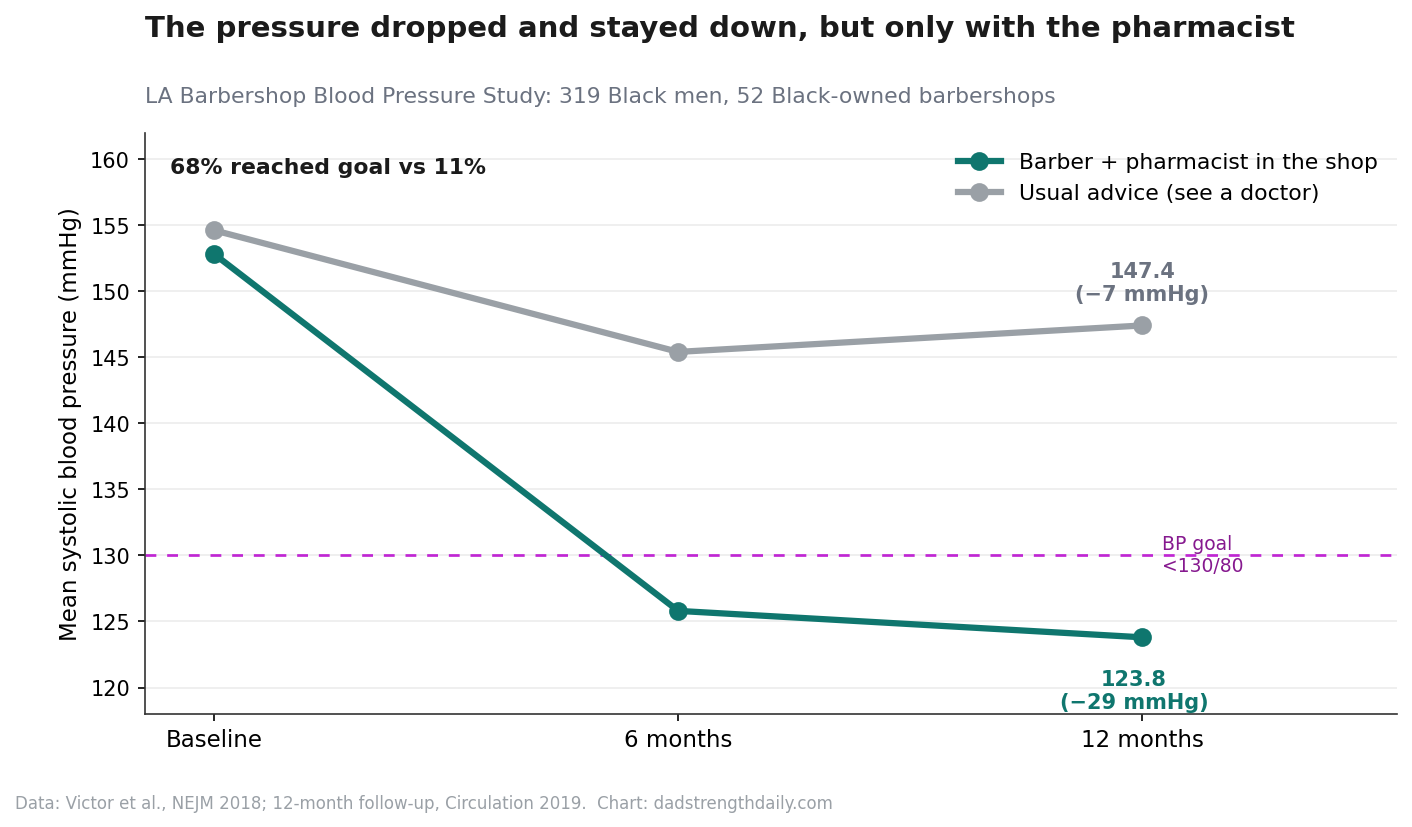
In 2018, a team led by Ronald Victor, a hypertension specialist at Cedars-Sinai, published a trial in the New England Journal of Medicine that enrolled 319 Black men with a systolic pressure of 140 or higher. They went to where the men already were: 52 Black-owned barbershops around Los Angeles, regulars who’d been coming in every couple of weeks for years.
Then they split the shops in two. In half of them, the barbers told their customers to eat better and go see a doctor, which is the advice everyone gives and almost everyone ignores. In the other half, they did something stranger. They handed the men off to a pharmacist who came to the shop, took their pressure, prescribed real medication under an agreement with their doctors, drew blood on the spot to check their kidneys, and kept showing up, haircut after haircut.
The difference wasn’t subtle. The men working with the pharmacist dropped their systolic pressure, the top number, by 27 points on average, from the low 150s down to about 126, in six months. The ones who just got the pep talk dropped about 9. By the end, nearly two-thirds of the pharmacist group had gotten under 130 over 80, against about one in nine of the others. Under 130 over 80 is the line at which doctors call blood pressure controlled. A year-long follow-up in Circulation showed it held: 68 percent still at goal, versus 11. And nine in ten men stuck with it the whole time, which basically never happens in trials aimed at hard-to-reach patients.
A 27-point drop isn’t a tweak. For the top number, that’s the gap between a quiet, decades-long grind on your arteries and kidneys and brain and a number that takes a lot of that risk back off the table. It’s bigger than what most blood pressure drugs pull off in a clinic, and they pulled it off in a barber’s chair.
Why it worked, and why that stings
The easy read is that the barbershop is magic. It isn’t. The story is delivery, not knowledge. We’ve known how to lower blood pressure for decades. The drugs are cheap and generic, and the pharmacology was never the hard part. The hard part is getting the right pills to the right person and keeping him on them, and for a lot of men the clinic is a bad place to do that.

One number in the paper stuck out. Forty percent of these men didn’t have a doctor who could even sign off on their prescriptions, so the researchers had to assign a community physician to cover them. Four in ten. Not men who’d missed a refill. Men who were outside the whole system, and the only reason anyone reached them is that the care walked into a room they already trusted and pulled up a chair.
The barber mattered because the barber had standing. An earlier version of this study from 2011 had barbers check pressure and point men toward a doctor, and it barely moved the needle, a couple of points. Trust by itself wasn’t enough. You had to carry the treatment, the pharmacist and the prescription pad, into the room people already trusted. Joseph Ravenell, an NYU doctor who’s spent his career on this and gave a TED talk about it, calls it meeting men where they are. Watch his eleven minutes if you want to feel why that’s more than a slogan.
I keep chewing on that, because it’s a quiet indictment of the rest of us. If a man’s pressure falls 27 points the moment you stop making him come to you, what does that say about how we built the clinic? The building, the appointment, the waiting room, the day off work: the whole setup screens out the people who need it most.
The part nobody pays for
The expensive part is human time. Each man got around seven in-person pharmacist visits in six months, plus calls, plus a small stipend for generic drugs and bus fare. Two pharmacists carried all of it. That’s a lot of skilled human time, and American medicine has no clean way to pay for it. Medicare doesn’t even count pharmacists as the kind of provider who can bill for managing a patient, so most of those hours generate nothing. The grant covered it. Grants end.
There were rough edges, and the paper owns them. Three men developed temporary kidney trouble, all on the same diuretic, a water pill, and it cleared up when they stopped it. That’s why there was a pharmacist and a point-of-care lab in the room, not just a barber with a cuff and good intentions. The authors also flag that the comparison wasn’t perfectly clean, since they were chasing a tighter target than the control group’s doctors probably were. The effect was big enough to survive every honest adjustment they made, and I’ll take a researcher who lists the weak spots over one who pretends there aren’t any.
What’s happened since says more. The model’s been checked for whether it pays off, and the math works by the usual standards. It’s turned up in Nashville, in a Kaiser program in Baltimore, even with NHS teams in the UK. The same idea has been aimed at diabetes, at clogged leg arteries, at HIV testing, at mental health, with barbers trained to listen for it. Newer trials are trying to catch men before their pressure climbs at all. A fluke doesn’t usually get copied, costed out, and built on like that.
Ronald Victor didn’t see most of it. He died of pancreatic cancer in late 2018, a few months after the trial he’d spent a career building toward finally ran in the biggest journal in medicine. His colleagues carried it forward, which is more or less how this kind of work happens: slowly, over years, by more than one person.
What we keep choosing instead
I don’t want to turn this into a feel-good story where the barbershop is a clever hack for everybody and the specifics melt away. This worked because Black men in this country carry the heaviest blood pressure burden of any racial, ethnic, or sex group, with the highest rate of hypertension-related death and lower rates of getting it treated and controlled, and they’ve got the best historical reasons of anyone to keep medicine at arm’s length. Somebody finally built care around that instead of wishing it away. I’m not part of that world, and I’m not going to write about it as if I am.
What the study runs on is something you can see from outside it: a barbershop holds men in a way almost nothing else in their week does. They come back. They talk. They drop their guard a little. Most of us don’t have a room like that. I don’t have a place I turn up to every two weeks where someone would notice if I started looking off, where the talk might wander toward the noise in the car I keep meaning to deal with.
What gets me is smaller and angrier than the usual takeaway. It’s not that you should go find a barbershop. It’s that we already know how to do this and mostly don’t. The drugs that dropped these men 27 points cost pennies. The expensive part was a pharmacist who kept showing up, and that’s the part nobody wants to pay for. There’s no billing code for blood pressure in a barber’s chair. There’s barely a billing code for a pharmacist doing it anywhere.
Meanwhile we’re pouring billions into unproven longevity supplements and research-chemical peptides that have barely been tested in people, a lot of it sold by subscription to men who already have a doctor they could call. I get the pull. A new molecule is a story you can own and sell. A pharmacist driving out to Inglewood every couple of weeks isn’t. But if the point is to add healthy years to the most lives, and not just to the lives that were already going to be fine, this trial has better evidence behind it than almost anything in the supplement aisle, and it’s been sitting in plain sight since 2018.
I bought my cuff. I take my telmisartan. I got there late, on my own, with every advantage, and it still took me years. It shouldn’t take that much advantage, and we’ve got the proof it doesn’t. What we seem to have decided is that proving it was the finish line, and that scaling it is somebody else’s job.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.