

The tabloids are calling it the cure for “Ozempic butt.” But it saved lean mass on a scan, not strength, and the real fix is still protein and a barbell.
I take tirzepatide. I’ve also lost a lot of weight on it, and the one thing I worried about the whole way down was muscle. Everybody on these drugs hears the warning eventually: a big chunk of what you lose isn’t fat. So when a new drug showed up last week pitched as the fix for exactly that, I read the actual paper instead of the headlines.
The drug is apitegromab, and the study, published in Nature Medicine on June 8, is the kind of result that’s easy to oversell. The short version is that it did one thing well and left the bigger question wide open.
Same weight off, more lean mass kept
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
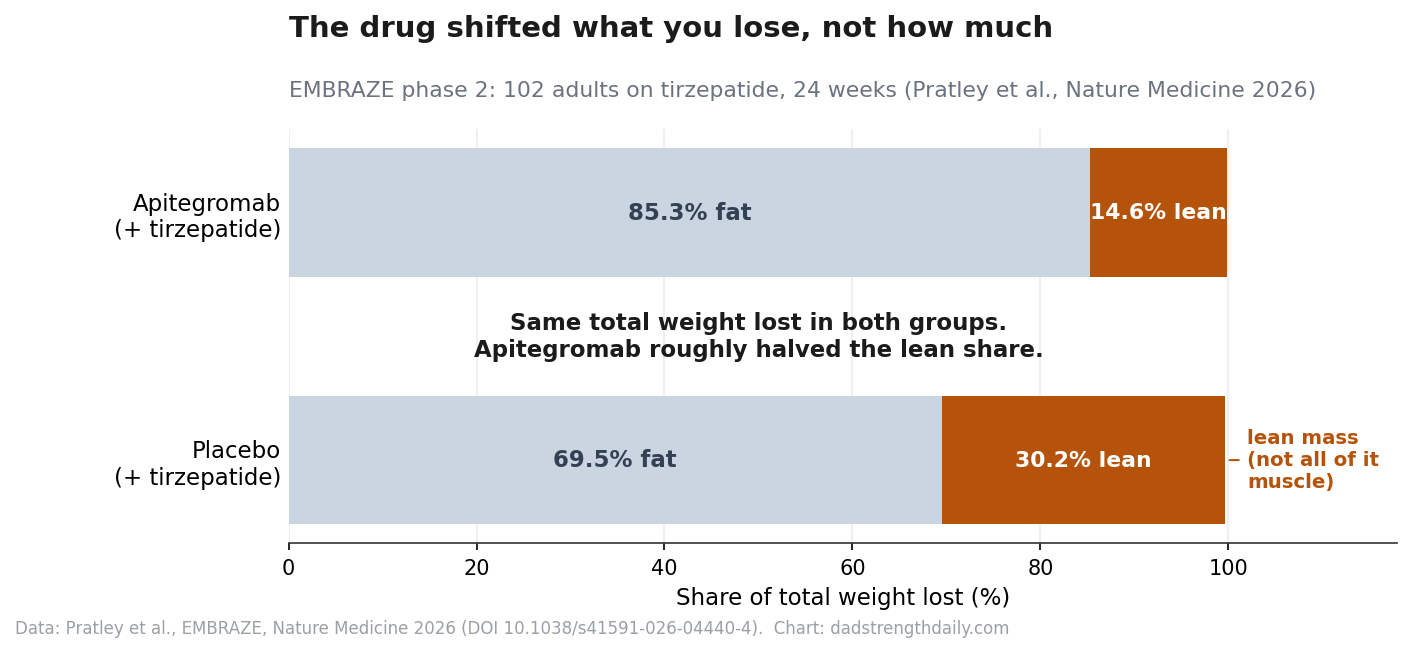
Researchers gave 102 adults tirzepatide, the drug in Mounjaro and Zepbound, and split them in two. Half also got apitegromab, an antibody that blocks myostatin, a protein that puts the brakes on muscle growth. Half got a placebo alongside their tirzepatide. After six months, both groups had lost about the same total weight. But the apitegromab group held onto more lean mass. They lost 1.9 kg less of it than the placebo group, which works out to keeping a little over half of the lean tissue they’d otherwise have shed.
That’s a real result, and it’s exactly the worry a lot of people on these drugs have been carrying. If you’ve watched someone get thin and somehow frail at the same time, you understand why it matters. Roughly a quarter to 40 percent of the weight people lose on these drugs is lean mass, not fat, and muscle is a lot harder to put back than fat is.
The lean mass it saved is real on the scan. Whether that scan number is muscle you can actually use is the part they couldn’t show.
The number that didn’t move
What improved here was lean mass on a body scan. That is not the same thing as being stronger, and they looked. They tested muscle strength with a handheld gauge and counted how many times a person could stand up from a chair, and at both six and eight months there was no notable difference between the apitegromab group and the placebo group. The drug kept the number on the scan up. It did not, in this study, show anyone getting measurably stronger. A 102-person, six-month trial might be too small to catch a real strength gain, but the honest read is they haven’t shown one yet.
That gap isn’t a quirk of one trial. The whole class of myostatin-blocking drugs has spent years running into it. You build muscle you can see on a scan, and the strength doesn’t reliably follow. An older review put the question right in its title: does muscle mass equal muscle strength? The answer, over and over, has been “not as much as you’d hope.” Bimagrumab, the best-known drug in this family, built mass without a clear strength benefit.
In fairness, apitegromab isn’t only a weight-loss drug. Its main job is treating spinal muscular atrophy, a genetic disease that wastes muscle in children, and there, on that disease’s movement tests, it genuinely helped kids move better. So the molecule can do more than pad a scan. But a child whose muscles are failing from a motor-neuron disease is a very different situation from a fifty-year-old shedding pounds on a weekly shot, and the company is leaning on that childhood-disease success to argue the drug has broader promise. The weight-loss data, for now, is a body-composition win with no function benefit behind it yet.
The fat loss wasn’t actually greater on the drug either, despite how some of the coverage framed it. Both groups lost about the same amount of fat. What changed was that a bigger share of the apitegromab group’s loss came from fat instead of lean tissue. The study was small, ran six months, was about 84 percent women, and was paid for by the company that makes the drug. It’s a promising proof of concept, which is what the researchers themselves called it. It is not a finished case. Naveed Sattar, a cardiometabolic specialist at Glasgow who wasn’t involved, told the Guardian it’s “too early to say whether this actually benefits people’s health or ability to move or function better.”
The fix nobody can sell you
Apitegromab isn’t alone, and it isn’t even the splashiest. Eli Lilly’s bimagrumab does something stranger. On its own it actually builds lean mass, and paired with semaglutide in a trial called BELIEVE, people lost far less lean mass than on semaglutide alone while losing more fat. Regeneron has one in the works too. This is becoming a drug category, and the hype is running ahead of the data. Mike Israetel, the bodybuilding scientist, sold the whole wave of body-composition drugs as the era of enhancement in a video that drew about as much ridicule as applause. The pitch is easy: GLP-1 drugs created a muscle problem, here’s a drug to fix it. The same unanswered question hangs over all of them. A better body scan, sure, but are you any stronger?
You’ll also hear that retatrutide, the triple-agonist coming up behind tirzepatide, spares more muscle on its own. Nobody has run that head-to-head, and retatrutide’s own body-composition substudy put the lean-mass share of the weight lost right in the range of the other drugs. The claim is running ahead of the evidence, same as the rest.
Step back, though, because not everyone thinks the muscle loss is worth panicking about. The crew at Barbell Medicine, who are usually careful with this stuff, argue the worry is partly overblown: the lean mass a DEXA scan counts isn’t all muscle you can flex, since it also includes water, glycogen and organ tissue; a lighter body needs less of it to haul around; and the trials rarely show people actually getting weaker. I take the point, and I still have my doubts. The loss is real, plenty of people on these medicines can feel it, and the industry obviously smells a market. Some muscle loss when you drop fifty pounds is normal. Losing more than you had to, when protein and a few hard sets would have saved it, is the part worth fixing.
And we already know how to hold onto most of it while you lose weight, no patent required. You eat enough protein and you do resistance training. That’s the whole protocol. Sattar, in the same breath where he called the drug early, said people on these medicines “should be supported to increase their physical activity,” because that “can help maintain muscle mass in a physiological way.” It’s the least exciting sentence in the coverage and the most useful one.
I’m a single case for it, and one person proves nothing, but it’s mine. I lost about 170 pounds on tirzepatide. A DEXA scan along the way showed I’d dropped 44 pounds of fat and added almost ten pounds of lean mass at the same time. I didn’t take a second drug. I ate a lot of protein and I trained, eventually with a coach five days a week. The drug quieted my appetite. Getting stronger was the boring part, the protein and the training, week after week, and no shot can hand you that yet. I wrote up how to handle the protein side here.
None of this makes apitegromab useless. If you’re older, losing weight fast, and physically unable to train, a drug that slows the muscle loss could turn out to matter, and longer trials will tell us whether the mass it saves becomes anything you can feel. I care a lot more about whether people end up stronger than whether the scan looks better. For most of us, though, the honest version is duller and cheaper than a second injection. For me it still means eating the protein and lifting the weights, the same as it did before this paper came out. The drug that does that for you is still a maybe. The one that already works is sitting in your kitchen and your garage.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.