
I have spent the last year and a half watching my own bloodwork change, and the number that moved the most was not the one I expected. My LDL cholesterol improved, which I was working on. But the marker that fell off a cliff was my hs-CRP, a measure of low-grade inflammation in the body. It went from 2.83, which is high, to under 0.2, which is about as low as that test reads. At the time I filed it under “inflammation down, good,” and did not think about it much beyond that.

Then a paper landed this month in the journal Cell that made me look at that number differently. A team led by Charles Swanton at the Francis Crick Institute in the UK described a set of 14 proteins in the blood that are elevated in people who go on to develop lung cancer, often more than five years before diagnosis. The thread running through those proteins is inflammation. (The New York Times wrote a good plain-language version of the study, if you want the short take.)
The headlines will be about the drug. I care more about something simpler. Lung cancer is the deadliest cancer we have, we still catch most of it too late, and more of it now hits people who never smoked. A test that flags risk this early is really about who gets screened, and who slips through the cracks now.
The 14 proteins showed up years early
The researchers took baseline blood from about 48,000 people in the UK Biobank, measured roughly 2,900 plasma proteins, and used machine learning to pull out 14 that track with developing lung cancer. None of these people had lung cancer when their blood was drawn. The team already knew who went on to get it, and went back to see what those people’s blood had looked like years earlier. Combined with age, smoking status, pack-years, and a history of COPD, the signature sorted the people who would go on to get lung cancer from the people who would not, and it did that better than the risk models doctors use now. (The measure here is AUC, which is just how cleanly a test separates two groups: 0.5 is a coin flip, 1.0 is perfect. This came in at 0.87, against about 0.77 to 0.81 for the current models.) The edge was biggest two to four years before diagnosis. They then checked it across eight more cohorts around the world, roughly 2,200 future cases and 54,000 controls, with blood drawn a median of seven years before diagnosis and in some people more than a decade out. It even held up in a Taiwan cohort that was almost entirely people who had never smoked.
That last part matters. A growing share of lung cancer now shows up in people who never smoked, exactly the people the current screening rules were never built to catch.
Detecting a tumor versus predicting one
Catching cancer early can mean two very different things, and they are not the same.
The first is detection: find a tumor that already exists. A low-dose CT scan does this for the lungs. Multi-cancer blood tests like Galleri do it by scanning for fragments of DNA shed by tumors into the bloodstream. I have taken one of these tests myself, and mine came back clear, which is reassuring. But the whole approach depends on there already being a tumor big enough to leave a trace.
This new research is the other kind, and it is a different idea entirely. It does not read a tumor. It reads the state of the lung, the soil, rather than the seed. What convinced me is that the 14-protein signature does not drop after a tumor is surgically removed. It is not measuring the cancer. It appears to be measuring the environment that lets cancer take hold.
And that environment is inflammatory. The 14 proteins rise when a specific inflammatory pathway, driven by a molecule called IL-1 beta, switches on. Smoking switches it on. Air pollution switches it on. The early cancer-driving mutations switch it on. The argument the authors make is that lung cancer is not driven by mutations alone. It is mutations plus a tumor-promoting inflammatory environment, working together. The same signature was also elevated in people who went on to develop COPD and pulmonary fibrosis, which points to a shared inflammatory soil sitting upstream of all three.
The “LDL for cancer” idea
Predicting risk is one thing. Doing something about it is another, and that is the part that got my attention.
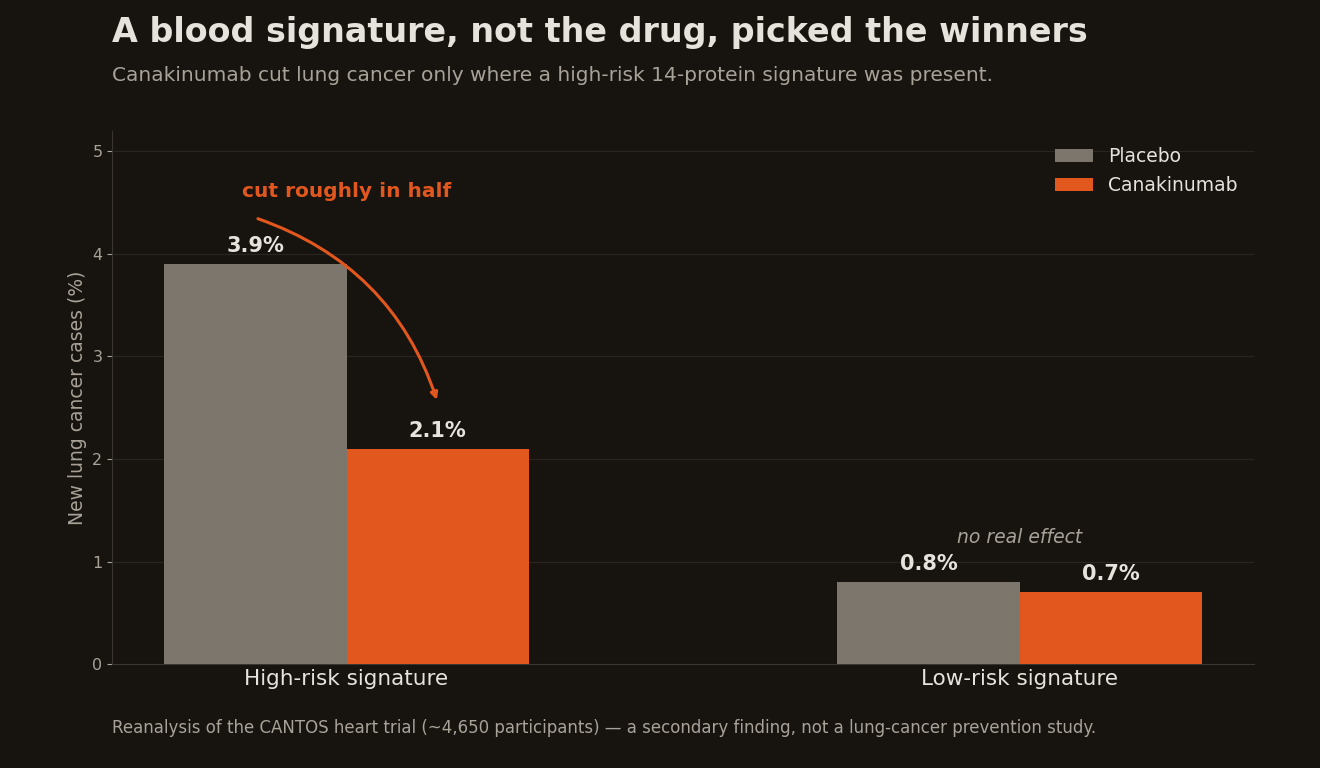
The researchers went back to a trial called CANTOS, which tested canakinumab, a drug that blocks exactly that IL-1 beta pathway. These were not random 50-year-olds. CANTOS enrolled people who had already had a heart attack and still had high inflammation. It was a heart trial. The drug only modestly reduced heart attacks, but it had a famous side finding that it also reduced lung cancer. In this reanalysis of about 4,650 of those participants, the effect was specific. Among people with a high baseline protein signature, canakinumab cut lung cancer incidence from 3.9 percent to 2.1 percent over the few years of the trial, roughly in half. In the low-signature group, it did essentially nothing.
One number in there is worth knowing, because it keeps prevention claims honest: the number needed to treat, or NNT, the number of people you have to treat to prevent one bad outcome. The lower it is, the more the treatment is worth. (I picked this up working through a course on how to read clinical research, part of teaching myself to read the studies instead of waiting for a headline to tell me what they said.) Here, the NNT to prevent one lung cancer fell from about 1,500 if you treated everyone to about 340 if you treated only the high-signature group. That does not make canakinumab a prevention drug. It is a potent immune-suppressing biologic that carries a real risk of serious infection, so even at an NNT of 340 it is something you would test in a trial, not hand out. But it is the difference between a drug nobody could justify and one worth studying in the right people.
So the signature may be more than a risk score. In this reanalysis it behaved like a responder score: it pointed to who actually benefited from the drug. Swanton’s own analogy was that this is “sort of an LDL for cancer,” the way a high LDL tells you who benefits from a statin. Given how much time I spend on ApoB and reading your own cholesterol panel, that framing lands for me.
Why I’m not ordering anything yet
I can already see this one getting hyped, so let me be clear about the limits.
It is discovery-stage. There is no blood test you can order for this today. Nobody has run a trial of canakinumab given specifically to prevent lung cancer. The CANTOS signal was a secondary observation inside a heart trial, and the drug has actually failed as a treatment for lung cancer that already exists. The window here is prevention, before a tumor, not therapy. And it is worth knowing that the senior author recently joined the board of Novartis, which makes canakinumab.
The near-term use is screening, not a pill
I don’t think this turns into a pill anytime soon. The practical use, if it holds up, is probably better screening. Right now a CT scan is only recommended for people 50 to 80 with a heavy smoking history, roughly 20 pack-years, who still smoke or quit within the last 15 years. That misses a lot of people.
Radon, secondhand smoke, and air pollution all cause lung cancer too, and a growing share of cases show up in people who never smoked and would never qualify for a scan. Meanwhile most lung cancer is still found late, after it has spread, which is exactly when it gets hard to treat. A blood test that flags risk years ahead could get more of the right people screened, including the ones today’s rules ignore.
What keeps nagging at me is the inflammation angle, and my own hs-CRP. I want to be careful here. hs-CRP is not one of the 14 proteins, it is not this test, and a dropping CRP is not a cancer screen. I cannot claim that losing weight lowered my cancer risk, because nobody has shown that. But hs-CRP and this signature are reading the same broad thing, inflammation, and it is starting to look like inflammation is something we can measure, and maybe lower, long before it turns into a disease. We have known that about heart disease for years. Watching that one number of mine fall, and then reading that the same family of inflammatory signals predicts lung cancer years in advance, made an abstract idea feel concrete.
I am not changing anything based on one paper, and I am not ordering a test that does not exist yet. What I am doing is watching this one closely, and keeping a question ready for my next physical: the day a blood screen like this is real, am I the kind of person who should be on it. The whole reason I pay attention to proactive health is the chance to catch a problem while it is still a number on a lab report, before it becomes a diagnosis. A test that predicts the deadliest cancer five years out, and points to who could be intercepted, is a real step toward that.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.