
The boring stuff still wins.
I’ll be honest up front: sleep is the corner of my own health where I’ve done the least. I can tell you what the research says, and I can also walk you through my own bedroom as the counterexample. My youngest spent long stretches wanting someone in the room until he fell asleep, which he only recently seems to have grown out of (fingers crossed!). My wife sleeps under one of those heavy blankets she loves (“so comfy!”), and I cook under it even with the AC set to 67. And most nights I fall asleep to a podcast on my phone in bed, which every sleep expert on earth will tell you not to do.
So this isn’t a victory lap. Before I read a single study, I did the thing I’d never bothered to do: I pulled a year of my own Apple Watch sleep data. And when I first looked, it flattered me. My REM seemed to be climbing, my nights seemed to be stretching longer, and I started writing this as a quiet little success story about how getting healthier had fixed my sleep too.
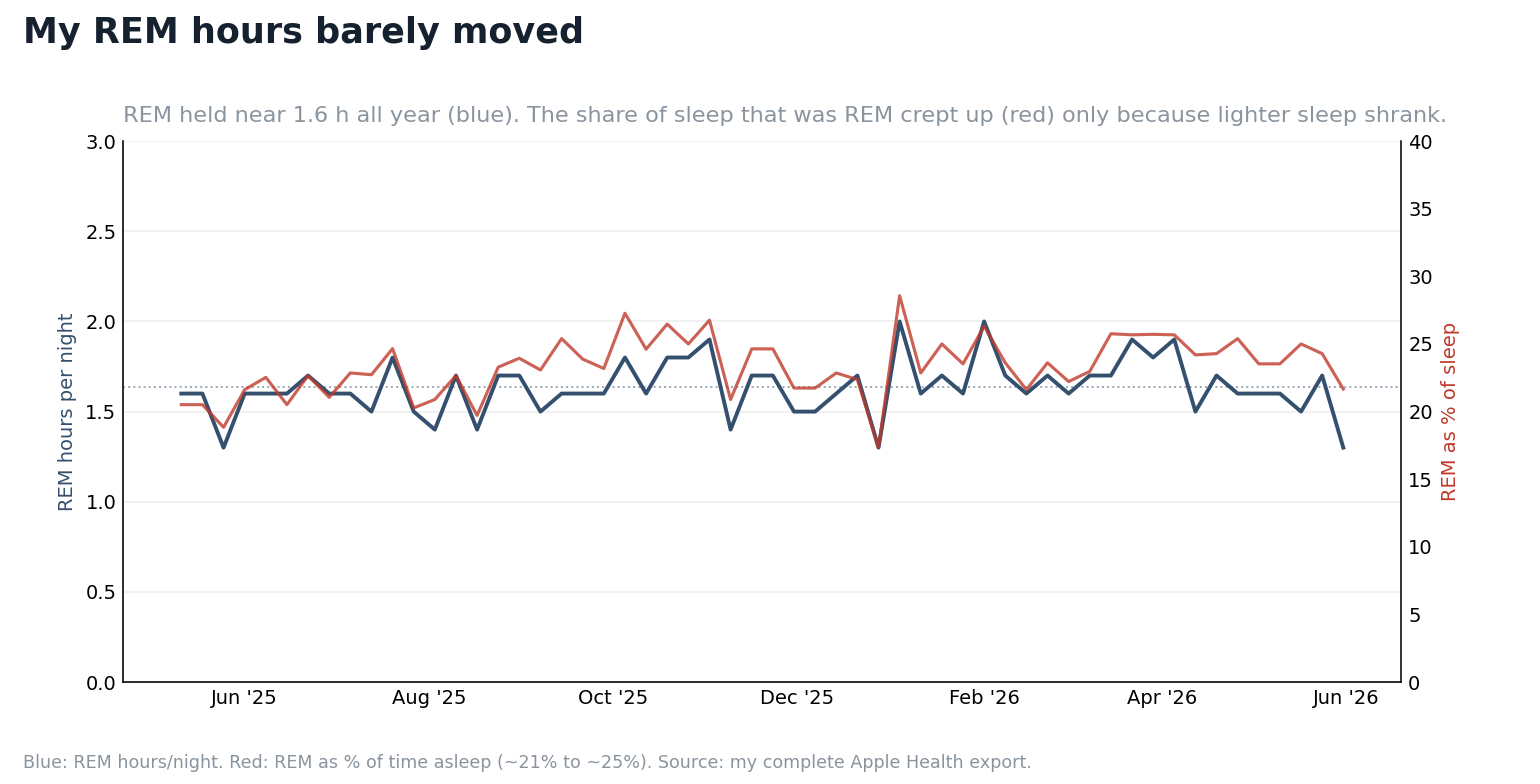
Then I re-pulled the complete export, recomputed from the raw stage data, and the flattering version fell apart. My REM had not really risen. My sleep had not stretched. It had been remarkably flat all year. That was a worse story, and a more useful one, and it is the reason I trust the boring advice in the rest of this piece more, not less.
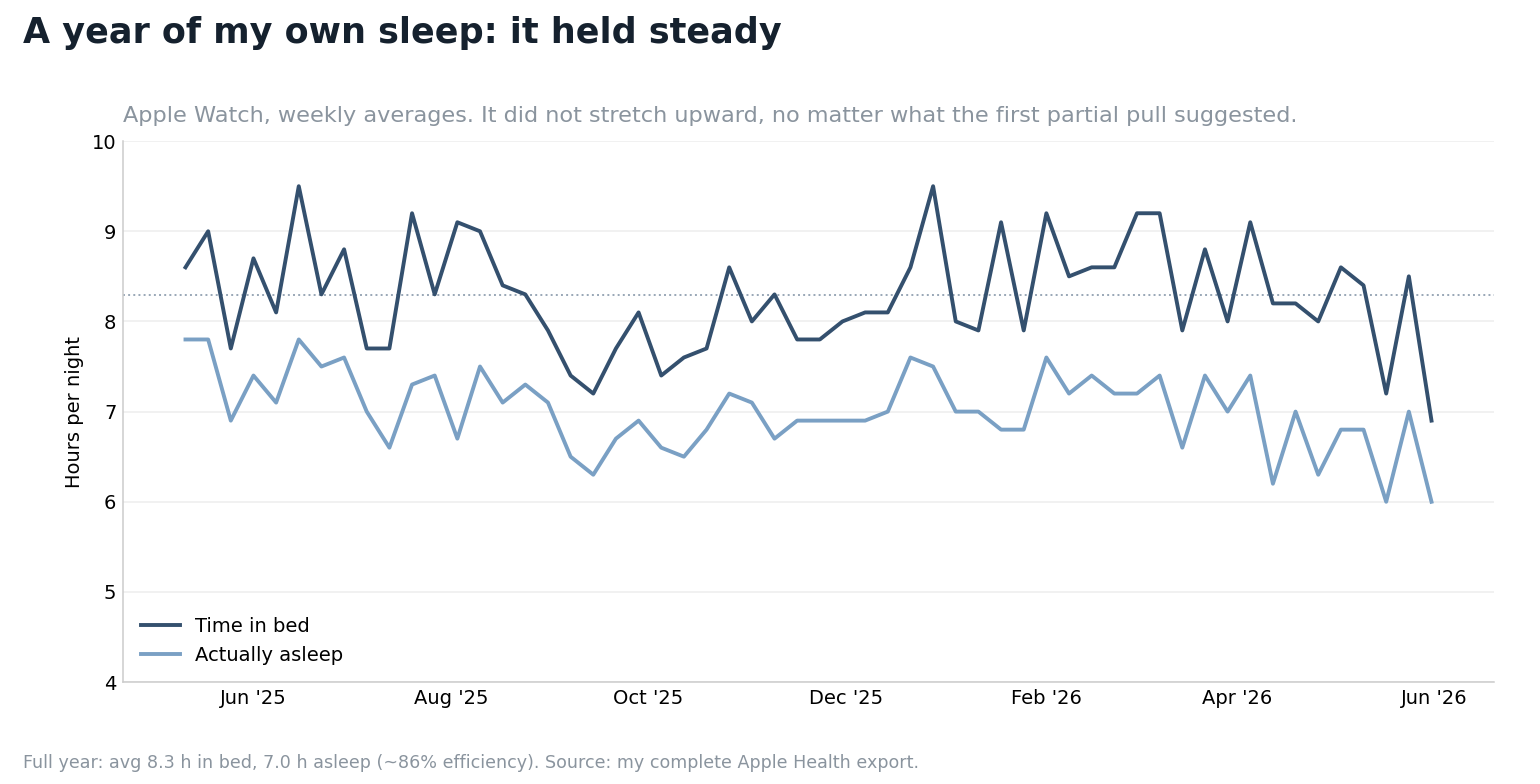
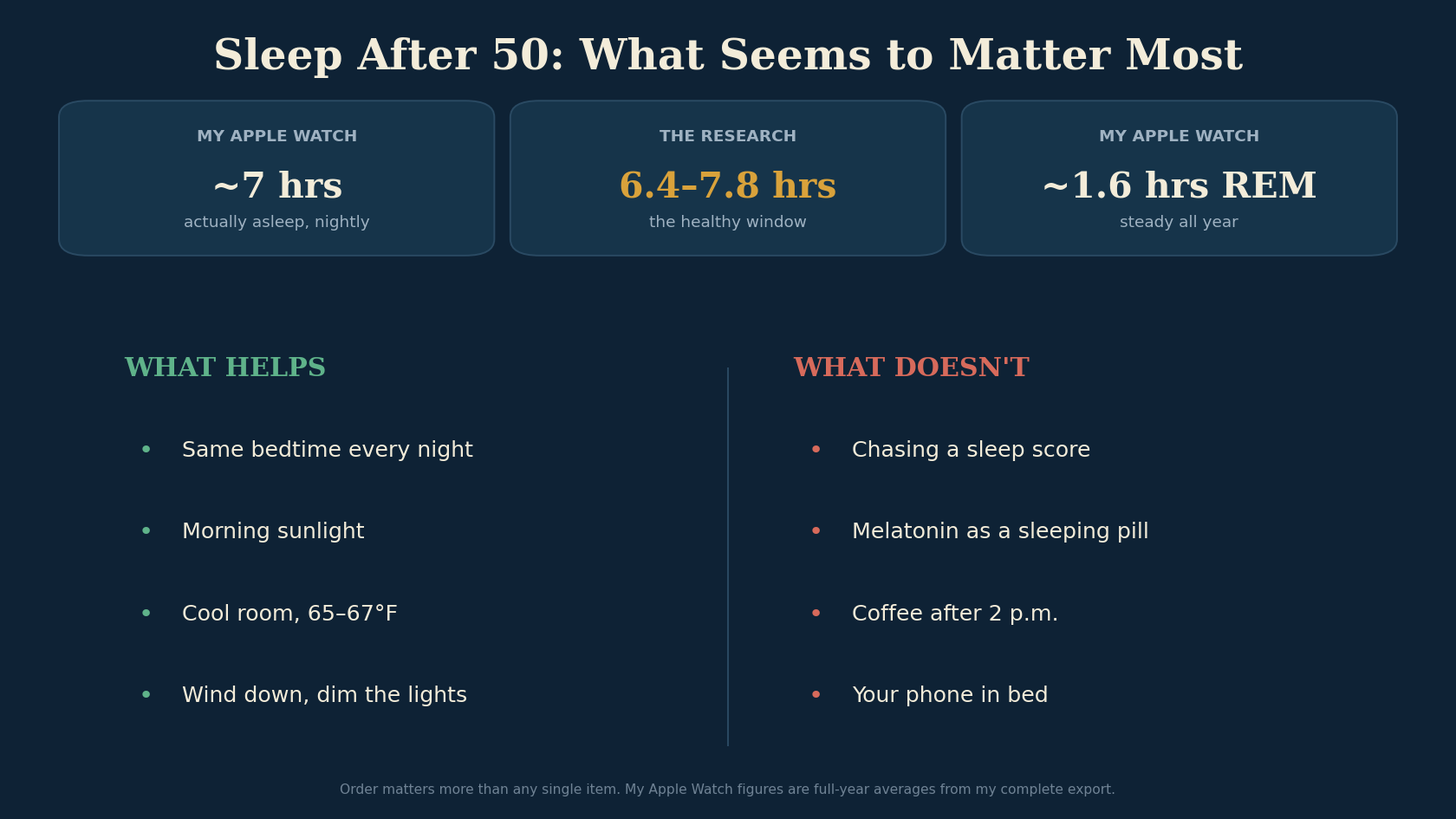
Here is what the full year actually showed. I average a little over seven hours of sleep, in about eight and a half hours in bed, steadier than I would have guessed. My REM held near an hour and a half the whole time. The only real drift was that my lighter “core” sleep shrank a little, which nudged REM’s share of the night up a few points without my making any more of it. The same data shows me waking at three in the morning more than I’d like, so I’m not holding myself up as a model. The honest shape of it is a flat line, not a climb.
And that flatness is the tell. My sleep didn’t quietly improve because I bought something or chased a sleep score, and it probably didn’t need a miracle. If anything, the full year pushed me back toward the boring explanation: the things that matter most are the ones that keep sleep from falling apart. When I finally read the research, that was exactly what it kept pointing at. If I had to rank the levers after all of it: a regular schedule first, then enough total hours, then morning light, then a cool room, then keeping caffeine and alcohol in their place, and only then, if a real problem survives all that, supplements or a prescription. Notice how far down that list the things people actually spend money on sit. The annoying conclusion is that the best sleep advice is the stuff nobody can sell you. The rest of this is the evidence behind that order, lever by lever.
The seven-hour window
One finding reframed it for me. Sleep duration sorts into a U: too little ages you, and so does too much.
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
It comes from a large new study that lined people’s reported sleep up against twenty-three biological aging clocks, measures of how old your body looks on the inside. Across every system and method, the people whose bodies looked youngest for their age clustered in a narrow band, somewhere between about six and a half and just under eight hours. Below that, the clocks ran fast. Above it, they also ran fast. Both short sleep and long sleep tracked with an older-looking body, more disease, and higher mortality. The sweet spot drifted a little by organ and by sex, but the shape held everywhere they looked.
The short-sleep side of that curve is intuitive. We have decades of data tying chronic short sleep to worse metabolic health, higher blood pressure, and blunted recovery, and most people reading this have felt it directly. Matthew Walker, the Berkeley sleep scientist, points out consequences, too: habitual short sleepers catch colds at markedly higher rates and mount a weaker antibody response when they get a vaccine. The long-sleep side is the part that trips people up, because the wellness optimization instinct is that if seven hours is good, nine must be better, and the answer is no. Sleeping nine or ten hours puts you back into elevated-risk territory, the same side of the curve as five.
It is also exactly the kind of finding that gets oversold. The data is observational, and the sleep numbers are self-reported, which means the headline almost certainly overstates the long-sleep danger. The cleaner reading is that long sleep is often a symptom, not a cause. People who are already sick, already depressed, already carrying an inflammatory burden tend to sleep more, and that underlying illness is what’s aging the clocks. The study itself hints at this, noting that the aging markers themselves seemed to partly account for the link between long sleep and late-life depression. A biological age clock is a useful mirror, but it’s only a mirror. It reflects the underlying health; it doesn’t create it. If you’re sleeping ten hours and waking up exhausted, the move is to find out why, not to set an alarm and force yourself to six.
For a man around fifty, one cause is worth ruling out before anything else: obstructive sleep apnea. If you snore heavily, wake up unrefreshed after a full night, get morning headaches, or your partner has watched you stop breathing and gasp back awake, that is not a willpower problem or a supplement problem. It is a plumbing problem, it gets more common with age and weight, and untreated it drives up blood pressure and cardiovascular risk while fragmenting exactly the deep sleep the rest of this piece is about. The first move there is a home sleep study, not a melatonin gummy or a cooling mattress. Worth flagging if you are on testosterone, too, since TRT can worsen untreated apnea in some men.
Walker adds one wrinkle I hadn’t considered. Bad sleep disguises itself as long sleep, because people who sleep poorly lie in bed longer trying to make up for it, and it’s the quality, not the hours on the clock, doing the harm.
So there’s a window, a bit north of seven hours for most adults, and the whole job is to land in it most nights, not to chase a sleep score or bank a surplus of hours nobody can actually save.
A steady schedule and morning light set the clock
If duration is the lever everyone already argues about, regularity is the one almost nobody markets, and it may matter more. Sleep scientists don’t even score sleep as a single number; they rate it on several dimensions, with timing and consistency counted alongside how long you slept.
A 2024 analysis out of the UK Biobank made this concrete. Researchers tracked around sixty thousand people who wore accelerometers, the wearable motion sensors, scored how consistent each person’s sleep timing was from day to day, and then followed who died. The people with the most chaotic schedules were more likely to die during follow-up than the ones who simply slept a little less, of heart disease and cancer especially, and the gap held up after accounting for how long they slept. That one got my attention, because going to bed at the same time is the least sexy advice in wellness.
That made sense to me, because regularity is the exact thing that shifted when I got deliberate. I wasn’t sleeping more. I was sleeping on a schedule. The body runs on a roughly twenty-four-hour clock that governs hormones, body temperature, glucose handling, and alertness, and that clock takes its cues from when you reliably do things, light especially. Drag your bedtime two hours later on Friday and Saturday and you’ve effectively flown yourself to a different time zone and back every weekend. People call that social jet lag, and the name strikes me as accurate. Your physiology treats it like the real thing.
Light is how you actually set that clock, and it’s the lever I’d been ignoring. Your brain reads morning light as the signal that the day has started, so getting outside in the first hour after you wake, even under a gray sky, anchors the whole rhythm that follows. I am lucky, our bedroom has big windows facing east so I get the sunshine for free. The other half is the part most of us botch at night: bright indoor light and screens after dark tell that same clock it’s still daytime and quietly push your sleep later. You don’t need a sunrise alarm or a lux meter. Get real light on your face early, dim things down in the last hour or two, and you’ve covered most of what the expensive circadian gadgets are selling.
The odd part, if you’re chasing optimization, is that regularity is free and unglamorous. There’s no device to buy and no supplement to take. You pick a bedtime and a wake time you can actually hold, and you stick to them, weekends mostly included. The wake time matters more than people expect, because anchoring when you get up and get light tends to pull the rest of the schedule into place behind it. I’d rather see someone with a rock-steady seven hours than a ragged eight.
What the brain clears out at night
What grabbed me is what the brain seems to do with the downtime: clean out its own trash. In a 2013 study in mice, the spaces between brain cells widened during sleep and cerebrospinal fluid washed through far more actively than during waking, flushing out metabolic byproducts. Researchers named this overnight plumbing the glymphatic system. One of the byproducts it clears is beta-amyloid, the protein that builds into the plaques associated with Alzheimer’s.
There’s human data pointing the same way. In a 2018 study, a single night of total sleep deprivation raised beta-amyloid signal on brain imaging in healthy adults. One night. And over the long term, poor and short sleep in midlife keeps showing up as a risk factor for later cognitive decline and dementia. None of this is settled, though, and anyone selling a pill to optimize your “glymphatic flow” is getting ahead of the science.
The bedroom is a temperature problem
The most underrated lever in my own house is the thermostat, and I know it because I lose the fight every night. Your core temperature has to fall a little to drop you into sleep and keep you there, which is why a cool room helps and a warm one wrecks you. It’s also why a warm shower an hour before bed works as well as it does: heating your skin pulls blood to the surface and sheds heat, so your core drops faster afterward. Researchers keep landing on 65 to 67 degrees for the room, though bedding, a warm partner, and body size nudge that, so treat it as a starting point. The real rule is simpler: cool enough that your core can drop and you don’t wake up sweating. I keep the AC at the top of that range, except my wife sleeps under a heavy weighted blanket she loves and I end up trapped under it, sweating. The blanket stays, because she sleeps better with it. The problem is mine: my half of the bed runs too hot.
That gap is what the temperature-regulating mattress covers are built to close, the Eight Sleep being the one everybody seems to own, or at least be sponsored by. I’ve been tempted, and the idea is sound: cooling the surface in the first half of the night lines up with the physiology, and separate zones solve exactly the standoff I’m describing. But before anyone drops two thousand dollars on a gadget, it’s the expensive version of a free thing. Most of the benefit is in the thermostat, a kicked-out foot, lighter bedding on your side, and a cool-down before bed. Buy the pod if you want it and can swing it. Just don’t buy it thinking the cheap version doesn’t work, because for most people it does.
The supplement aisle and the pharmacy counter
The supplements and the pills are where most people start, and they’re where the evidence is thinnest.
Start with the thing that has the best evidence and the worst marketing, because nobody profits from it. For chronic insomnia, the first-line treatment in the actual clinical guidelines isn’t a drug. It’s cognitive behavioral therapy for insomnia, a short structured program that retrains the habits around sleep, and it beats sleeping pills over the long run without wearing off when you stop. Ask your doctor for CBT-I by name or use a validated digital program. It’s less convenient than swallowing something, which is exactly why it gets ignored.
The supplements people actually buy are a step down from that. Melatonin is the most misunderstood: it is a timing signal, not a sedative, useful in a small dose, well under a milligram, for a clock that is off, like jet lag or shift work, and useless as the nightly sledgehammer the five and ten milligram gummies are sold as. Magnesium, valerian, ashwagandha and the rest are mild and inconsistent, cheap and harmless, useful ideas rather than magic.
Here’s my own n of one. I take magnesium threonate and after months honestly can’t tell it does a thing. Glycine surprised me, though, quicker to drop off and a little deeper, almost the first night. That’s an anecdote, and the trials behind it are small and soft, but it’s the one thing in this section I’d actually notice if it disappeared.
A few common aids are worse than nothing. The “PM” painkillers and most over-the-counter sleep tablets run on a sedating antihistamine, usually diphenhydramine, where heavy long-term use in older adults tracks with higher dementia rates. Alcohol is the most popular sleep aid in the world and one of the worst: it gets you down faster, then fractures the back half of the night and suppresses REM. And caffeine has a five-to-six-hour half-life, so the afternoon cup is still working at bedtime, thinning your deep sleep whether you feel it or not; if your nights are shaky, stop by early afternoon.
Then there’s the actual pharmacy, which belongs with a doctor. The old workhorses, the benzodiazepines and “z-drugs” like zolpidem (Ambien), sedate you rather than hand you real sleep and bring tolerance and dependence, so they’re best as a short bridge through an acute stretch, not a nightly habit. The newer prescription options are genuinely more interesting, enough that I’ll give them their own post. If you want to go deeper now, Peter Attia’s deep dive on sleep pharmacology is the best long-form treatment of the whole drugs-and-supplements question.
One aside, since I’ve leaned on Walker more than once. His book Why We Sleep got a lot of us taking sleep seriously, but a detailed fact-check by Alexey Guzey catalogued a long list of errors and overstatements that Walker only partly acknowledged. Read it for the motivation, and discount the scariest numbers.
The order that actually matters
Most people have this backwards. The schedule and the obvious wreckers, the late alcohol, the irregular nights, the bright screens, come first. Supplements are a maybe. The pharmacy is for real insomnia that survives all of that, with a doctor helping you weigh it.
I’m not a perfect sleeper, and this piece isn’t pretending otherwise. The kids still wake up, I still cook under that blanket, and I still drift off to a podcast on a phone that’s supposed to be charging in another room. Walker’s real objection isn’t the screen light, it’s that a phone on the nightstand trains your brain to expect the day’s stress waiting there, which lightens your sleep all night. I know he’s right. But a quiet voice in the dark is the one thing that stops me lying there rehearsing tomorrow’s work, and at eleven p.m. that trade keeps winning.
What I did change was smaller, and it stuck. I’m in bed by nine most nights now, unless a late work meeting or a kid runs long, and I wake up on my own before the watch buzzes at 5:45. Nine sounds early until you remember the old line about sleeping when the baby sleeps, which still works with older kids: I just go down when they do. Weekends mostly hold, and most mornings I’m up before the alarm. The blanket and the phone are still winning.
The bedtime was the part I could fix.
A note on the data (June 2026): an earlier version of this post reported a bigger rise in my REM and total sleep than the full numbers support. The figures and charts here reflect my complete Apple Watch export, recomputed from the raw sleep-stage records; the earlier version drew on a partial pull that overstated the trend. Which is its own small lesson, and the reason the boring advice above gets the spotlight instead of my data.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.