
I get prescriptions online, and most of the time I like it. I fill out the form, answer the questions, and the medication shows up at my door, no half day lost to a waiting room. I am not anti telehealth. I use it, I tell my primary care doctor about everything I get this way, and when it makes sense I move the prescription over to her so insurance covers it. The access benefit is real.
What bothers me is the flip side. The same system that works for me, because I read this stuff obsessively and know who to loop in, is built to turn a television ad into a prescription for someone who never sees what happens behind the screen.
And what is happening behind the screen is stranger than I expected. Reporters at STAT documented a clean example. A patient fills out the intake on the website for Addyi, a prescription drug for low libido, and gets Addyi. The same patient, with the same profile, fills out the intake on the website for Vyleesi, a different drug for the same condition, and gets Vyleesi. Both prescriptions were written by the same nurse practitioner, at the same affiliated medical group, off intake surveys that were identical except for the final drug specific questions. The website effectively chose the drug, and the clinical encounter rubber-stamped it.
If you are a man somewhere in your forties, fifties, or sixties, this machinery is already in your Instagram feed. Weight loss shots, testosterone clinics, ED pills, hair loss subscriptions, sleep aids, peptides. Some of it is real care that happens to be convenient. Some of it is a sales funnel in a white coat. From the outside they can look identical.
So I wanted to understand how a system that does that got built, and how to tell, from my own couch, when I am looking at an actual clinic and when I am looking at a sales funnel. The answer is not really about any one company. It is about a legal structure almost everyone in this market uses, and what happens when you bolt a marketing machine onto it.
There is a simple way to tell the two apart, and it does not take a single study. Does the service ever say no, or does every visit end in a prescription? Does it ask for real information, labs and history and a conversation, or the same short survey no matter what you want? Can you find out who is actually prescribing, and where the drug is made, or is that buried? Those three questions are the whole consumer test. The rest of this is the story of why a system grew up that makes them so hard to answer.
The doctor you didn’t quite see
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
When you order something online and a prescription appears, the company whose ad you saw did not write it. In more than thirty states it is illegal for a corporation to practice medicine at all. A corporation cannot hold a medical license or make the clinical call, and it cannot be the prescriber.
So telehealth companies split themselves in two. One half is the brand you recognize, which the lawyers call a management services organization, or MSO. It owns the website, the software, the marketing, the checkout, the customer support. The other half is a separate professional corporation, a PC, that is owned on paper by a physician and actually employs the clinicians who prescribe. The PC is supposed to be a firewall. The idea is that medical decisions stay with the doctor and never get bent by the corporation’s need to sell more product.
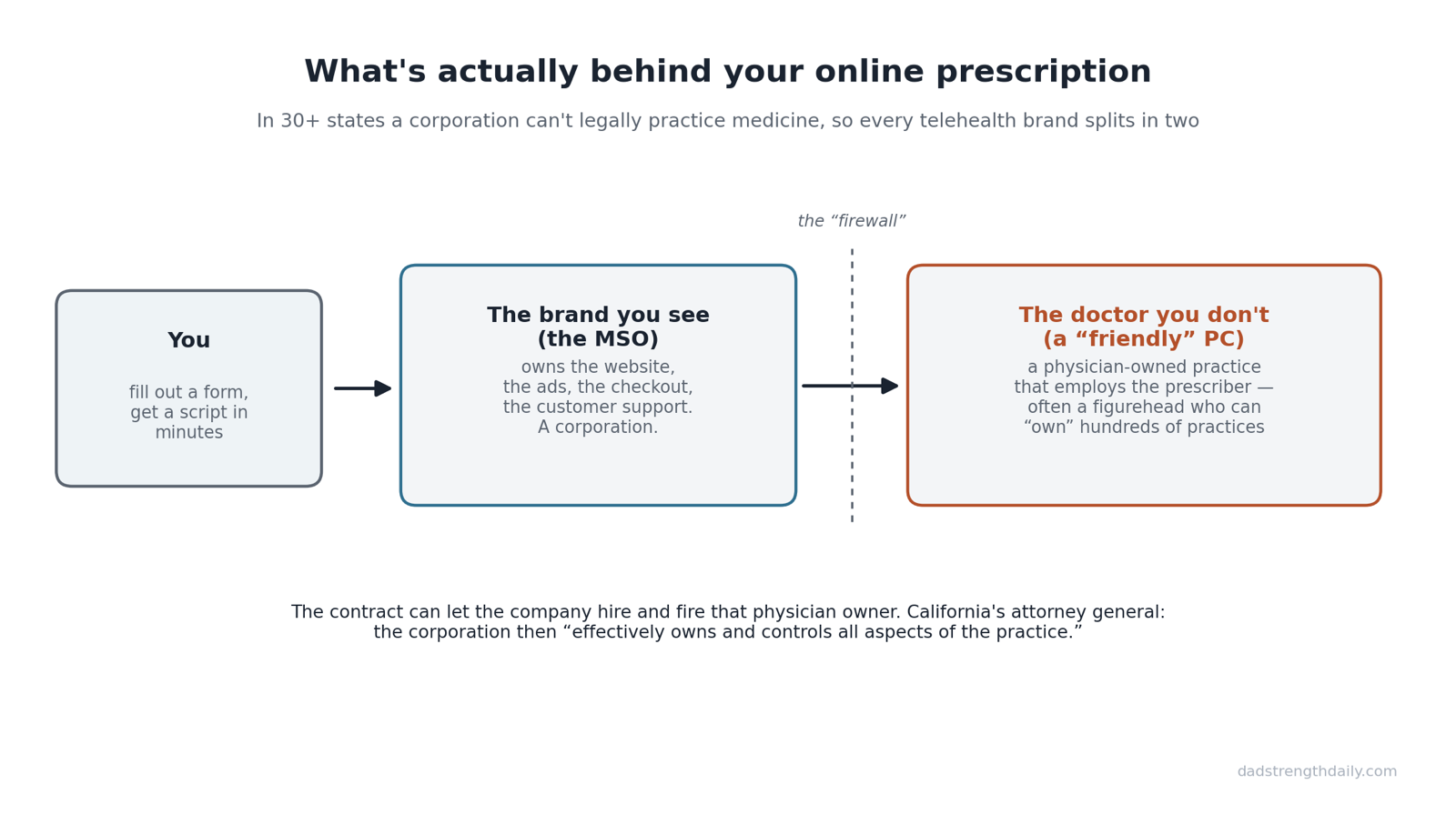
The brand owns the front door. The medical group holds the license. The contract decides who is actually in charge.
That is the theory. In practice, the firewall is often thinner than it looks. The doctor who owns the PC can be a figurehead. The Milbank Memorial Fund, in a 2025 brief by health policy researchers at Brown University, describes how an MSO can “assume de facto ownership of the medical practice by installing a friendly or captive physician owner,” a licensed doctor who, as the brief puts it, “answers to the corporate MSO.” The contracts do the work. They can give the corporation the right to replace the physician owner, or make it impossible for that owner to walk away without losing the practice.
California’s attorney general made the same point in a March 2026 court brief, and he was blunt about it. When an agreement lets a corporation replace the physician owner with a doctor of its choosing, he wrote, “the corporation effectively owns and controls all aspects of the practice.” On paper a licensed physician is in charge. In reality, the brief notes, that physician is often an employee of the thing he supposedly owns.
If this sounds like a fringe arrangement used by sketchy operators, it is not. It is the plumbing under much of the industry, including the respectable parts. Amazon paid 3.9 billion dollars for One Medical, a primary care company with real clinics and hundreds of thousands of patients. Amazon owns the management company, 1Life Healthcare. The doctors you see at One Medical work for affiliated physician owned professional corporations. Same structure. A New England Journal of Medicine piece on this trend warned, back when the Amazon deal was announced, that corporate investment in primary care could “reduce physicians’ clinical autonomy” and urged states to strengthen their rules against the corporate practice of medicine.
So the structure itself tells you almost nothing. A 3.9 billion dollar Amazon primary care brand and a checkout-style weight loss site can run on the exact same legal scaffolding. Which means the structure is not what you should be looking at. What matters is what gets built on top of it.
The four groups behind a thousand brands
So who is actually writing the prescriptions?
The big names, Hims and Ro, can afford to build their own networks of clinicians. Most of the market cannot. There are dozens of smaller sites you have never heard of, with names like Skinny Theory, Nu Image, and Max Weight Loss, and they get into business by renting. They plug into a ready made network of clinicians, what the industry calls a white label medical group, and they can launch in a matter of days. The brand you see supplies the ads and the checkout. The white label group supplies the doctors, and the same group can sit behind dozens of sites that look unrelated.
The renting is more concentrated than I would have guessed. When the FDA sent warning letters to more than seventy telehealth companies over how they marketed compounded weight loss drugs, STAT found that at least 30 percent of them traced back to just four medical groups: Beluga Health, OpenLoop, MD Integrations, and Telegra. One lawyer who advises these companies put the risk plainly. When regulators see the same medical group behind five different warning letters, she said, they do not see a coincidence, they see a supply chain.
And often you cannot tell who the group even is. A third of the warned companies did not name their medical group in their public materials. I went looking myself. I read the terms and privacy policies for several of these services. When I checked, in June 2026, CallonDoc, AlgoRx, and TelyRx did not name an affiliated medical practice at all. AlgoRx’s terms refer only to “licensed third party Providers” exercising “independent professional judgment,” which is the legal language for a firewall without telling you whose firewall it is. The doctor on the other end is not just behind the screen. He is behind a screen with the name scratched off.
The clinic and the vending machine
This is not really about good telehealth companies and bad ones. They run on the same parts. What differs is the kind of care built on top.
At one end you have something that behaves like an actual clinic. Marek Health, a men’s health and hormone service I have used, sits here. You get comprehensive lab work, an actual consult with a provider, and a protocol that looks at your thyroid and your metabolic markers, not just the one number you came in for. There is follow up. There is a relationship. It uses the same MSO and affiliated provider model as everyone else, but it uses it to deliver care.
At the other end you have something that behaves like a vending machine. On TelyRx you search a menu of four hundred plus medications, pick the one you want, answer a short questionnaire, and a licensed doctor reviews it without ever talking to you. AlgoRx offers what it openly calls a Shopify style checkout for medications. The clinical encounter is real in the narrow legal sense that a licensed person looked at your file. It is not real in the sense most patients assume, where a clinician works out what is wrong with you and decides what you need.
An obesity physician quoted by STAT called the incentive at that end of the spectrum a “humongous red flag,” one so misaligned that he could not imagine it would not produce profit driven prescribing rather than medical prescribing. The firewall is identical at both ends. What flows through it is not.
When the website picks the drug
The newest layer is the one that should worry you most, because it is the one designed to find you.
Drug makers have started building telehealth funnels around a single product. There are companies whose entire business is this. One, Prescribery, describes itself as “a telemedicine platform built for pharmaceutical brands.” Another, UpScript, provides telehealth onramps for dozens of drug and device makers. You see an ad for a specific drug, you click “talk to a doctor now,” and you are routed into a visit that exists to get you that drug. The visits are cheap on purpose. A consultation that might run forty five dollars drops to ten with a code, and sometimes the code runs right in the ad. The Addyi funnel used a ten dollar visit code, PINKPILL, that ran as an Instagram and Facebook ad.
Look at how that visit is structured and the Addyi versus Vyleesi story from the top of this piece stops being a fluke and starts looking like the design. The intake is a short survey. The review is asynchronous, meaning no one talks to you. The drug is set by which website you walked in through. And here is the tell on the economics, the question a health law professor asked when she looked at these arrangements: if the visits are this cheap, where are they making their money? A lot of these visits are also cash only by design. The free consultation for one prescription drug app comes with fine print barring you from submitting it to any insurer, which can help keep the transaction clear of the federal anti kickback rules, which mostly bite when a government program like Medicare is paying.
A group of United States senators put a number on how well this machine converts. A 2025 investigation into the manufacturer run platforms LillyDirect and PfizerForAll reported that 74 percent of LillyDirect patients who saw a telehealth provider walked away with a prescription, and 85 percent of PfizerForAll patients routed to one provider did. A normal doctor visit does not end in a prescription five times out of six. A sales funnel does.
This is also where my worry about ads stops being abstract. The funnel did not stay on my phone. It moved to the Super Bowl. Hims ran a weight loss ad during the 2025 game that the FDA commissioner later said violated drug promotion rules by selling the benefits and skipping the risks. By 2026 there were two of them, a Ro spot with Serena Williams and a Hims spot built around the gap between what rich and poor people can afford. These are not small targeted ads finding people who already went looking. They are the biggest stage in American media, used to create demand for a prescription drug category, pointed at an audience that is mostly not reading the studies.
Why the crackdown speeds it up
There is a crackdown coming, and it is real. I do not think it is the main story.
The FDA is sending warning letters. California’s attorney general is arguing in court that the captive PC contracts are illegal, backed by a new state law, SB 351, that explicitly extends the ban on corporate medicine to private equity and hedge funds. Oregon, Vermont, and Washington have all taken aim at the model, and the telehealth lobby has pushed back hard, winning carve-outs in two of those states and helping stall the bill in the third. Eli Lilly and Novo Nordisk are suing telehealth companies over how their compounded weight loss drugs got prescribed.
But none of that kills the model. It concentrates it. Compliance is expensive. Lawyers, audits, fifty state licensing, real clinician networks, all of it costs money the small renters do not have. As the rules tighten, the sites running on a borrowed white label group and a survey get squeezed out, and the business flows to the handful of players big enough to do it properly, plus the few large medical groups everyone else depends on. The crackdown does not end the industry. It picks the survivors.
Meanwhile the drug makers are selling straight to patients. Lilly launched LillyDirect in January 2024, and Novo followed with NovoCare in March 2025, both offering branded drugs for cash, a few hundred dollars a month rather than the four figure list price, shipped to your door. This part is friendlier to patients than the funnels above, and the details matter. Your own doctor can write the prescription and send it straight to the manufacturer’s pharmacy. That is what I did in 2024. My primary care doctor wrote my Zepbound prescription, and I filled it through LillyDirect at the cash price. What you cannot do is take that price to your corner drugstore. The discount lives inside the maker’s own pharmacy, and that is where the control sits. The prescriber can still be your own doctor, but the fulfillment and the price belong to the company that makes the drug. For patients who do not have a doctor, the same platforms will hand them one of the telehealth providers the manufacturer chose, which is where this quietly rejoins the funnel.
And the gray zone energy is already migrating to the next thing. As the compounded weight loss loophole closes, the same direct to consumer machinery is turning toward peptides like BPC-157, the molecule a whole separate corner of the wellness internet is selling as a research chemical while the FDA decides what to do with it. The structure does not disappear when one drug gets regulated. It looks for the next drug that is not.
So the crackdown changes who wins, not where this is going. The small operators get squeezed out. The big ones, the ones with the lawyers and the compliance budgets, come out stronger.
What you’re actually buying
What keeps nagging at me is how close a prescription is getting to a purchase. The clinical encounter, the part where someone who knows medicine works out what is actually wrong with you, is the expensive step the whole system is trying to automate away. Sometimes that is fine. Sometimes it is the only protection you have.
It is fine when you know what you have and you know what you need. A refill of a medication you have taken for years, a condition you already manage, a low risk drug with a clear protocol. A medical ethicist who studies these platforms calls that the real benefit, and she is right. For a patient who is informed and stable, skipping the waiting room is a gift.
It is a problem when the funnel is doing the diagnosing. The danger is not telehealth itself, it is the cheap drug specific visit out competing actual care. As one patient advocate put it, why would I choose the thirty dollar appointment over the ten dollar one if I do not even know the two are different? The harms are not theoretical either. As of mid 2025 the FDA had logged hundreds of adverse event reports tied to compounded versions of the weight loss drugs, though a report is a signal, not proof the drug caused the harm, and the agency says the true count is probably higher. That is on top of the cases it warned about from telehealth Adderall mills that ended in federal charges, and the privacy regulator has already fined one of these companies for piping patients’ sensitive health data to advertisers.
The three questions from the top are the ones I would give my own kids. Does it ever say no, or does every visit end in a script? Does it ask for real information, or run the same short survey no matter what? Can you find out who is actually on the other end, and where the drug is made? A real clinic will fail you sometimes, because saying no is part of the job. A funnel rarely will, because a no is a lost sale.
And then there is the thing that makes the whole arrangement work for me, which has nothing to do with being clever. I do not let the online transaction be the entire relationship. Whatever I get online, I bring to my doctor who sees the whole picture, who knows the rest of my chart, who can tell me when one thing I am taking quietly argues with another. The convenience is the front door. It should not be the whole house.
The access is real, and I will keep defending it. One thing about it still nags at me, though. The less homework a patient does, the better this sales operation works on him, and good medicine is supposed to run the other way.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.