
A Yale team posed as a qualified patient and tried to get GLP-1 weight-loss drugs from 49 online sellers. Forty-five wrote a prescription, often off little more than a form.
I take a GLP-1, the class of drugs people know as Ozempic, Wegovy, Mounjaro, and Zepbound. I also get some of my care online, and most of the time I like it. So when a new study landed showing exactly how easy it is to get one of these drugs from a website, I paid attention, because I have skin in this.
A few weeks ago I wrote about how online prescribing is built to work like a sales funnel instead of a clinic. That piece was mostly about the legal plumbing. This one is about what happens when researchers actually run the experiment. A team at Yale did, and the numbers are blunt.
What the researchers actually did
The Yale team did what a lot of patients do, except they took notes. One researcher posed as someone who qualified for a GLP-1 and went shopping across 49 direct-to-consumer sites between August and December of last year, a secret-shopper audit published in JAMA on July 6. The patient always picked the cheapest option. When a site wanted a full-body photo, it got only an upper-body one. If a site asked for blood work, the patient stopped there.
It is one stand-in patient, not thousands, so treat it as a careful spot check rather than the last word. But it is the closest thing we have to filming the vending machine while it runs.
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
Forty-five yeses, and how fast
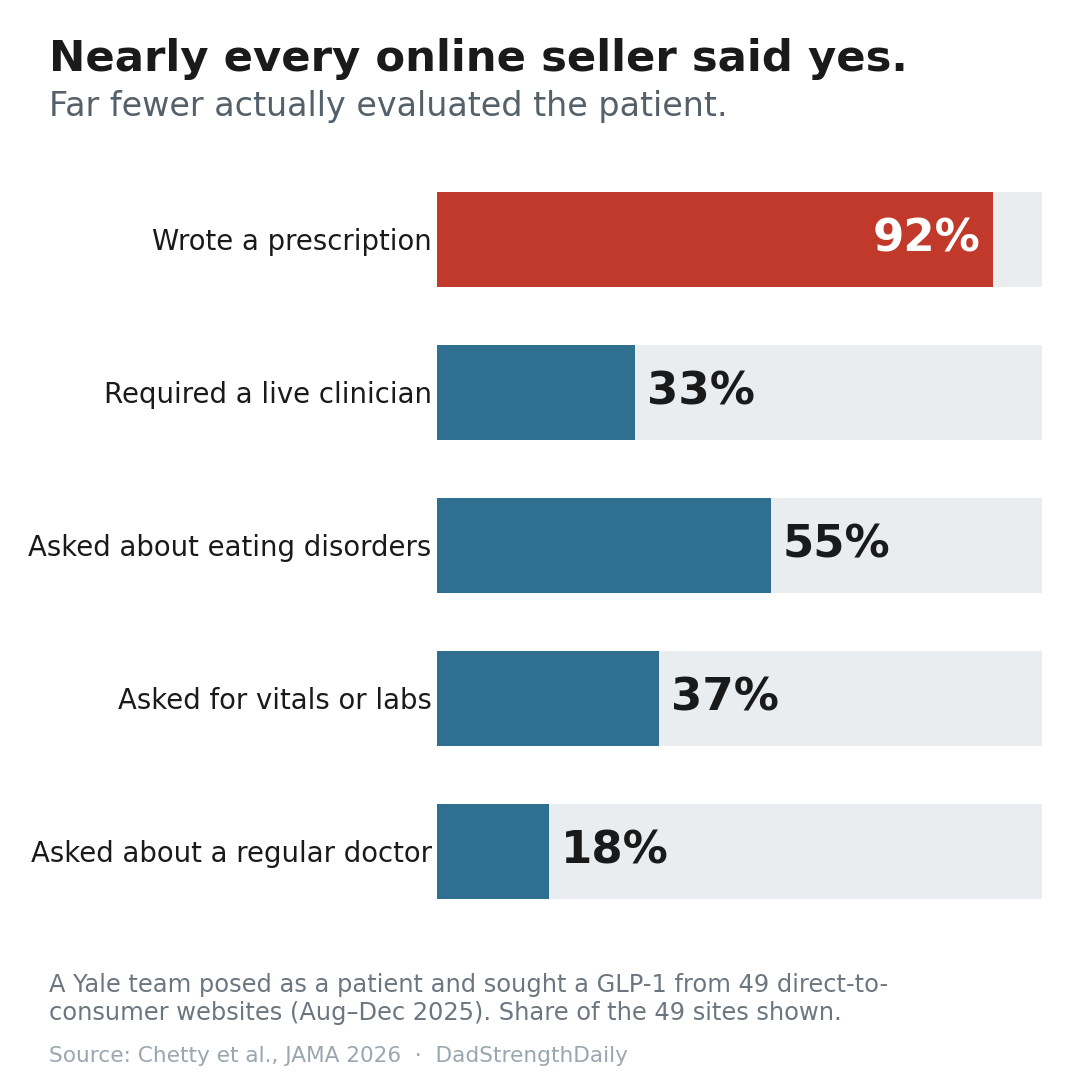
Of the 49 websites, 45 wrote a prescription. That is nearly 92 percent. Thirty-four of them mailed the drug. Only four said no, and two of those only balked because they wanted blood work first.
What got me was the speed. The typical time from questionnaire to prescription was a day or less. Two sites issued a compounded prescription in five minutes or less. Fewer than a third of the sites required you to talk to a clinician in real time, by video or phone. Only about one in four required a video visit, and when a visit did happen, the middle-of-the-road length was nine minutes.
So for most of these sites, the whole doctor visit was a form you filled out yourself.
The things a real evaluation would have caught
This is where it gets uncomfortable, because a GLP-1 is a real drug with real downsides for the wrong person, and the study measured how often basic screening simply did not happen.
Only about half the sites asked anything about eating disorders at all. That matters more than it sounds, since these drugs blunt appetite hard, and doctors have real worries about what happens when someone with a hidden eating disorder gets them. Only 37 percent asked for any patient-reported numbers like blood pressure or cholesterol. Fewer than one in five asked whether you even have a regular doctor.
The photo detail is almost comic. Nine sites, one in five, wrote the prescription off an upper-body photo even though their own rules asked for a full-body shot or a picture on a scale. And three quarters of the sites, 34 of them, automatically charged the card and shipped the drug without asking the patient to confirm anything first.
A few sites even had an internal database flagging that this same patient had already gotten a prescription elsewhere. One of them denied the order for that reason, then reversed itself and prescribed anyway after the patient asked for a refund.
This is not an argument against telehealth
The easy read here is “online medicine bad.” That is not what I take from this.
I manage my testosterone therapy through an online clinic. They run my actual bloodwork, they adjust my dose off the labs, and there is a real person on the other end when something looks off. That is telehealth working the way it should. The difference between that and what this study describes is not the screen. It is whether anyone is genuinely evaluating you, or whether the site has quietly decided the answer is yes before you finish typing.
Most of the drugs in the study, about 87 percent, were compounded versions, meaning pharmacy-made products that are not FDA-approved the way Ozempic, Wegovy, Mounjaro, and Zepbound are. That does not automatically make them fake or unsafe, but it does mean the usual FDA review never evaluated that finished product. Six in ten of those came bundled with extra vitamins the patient never asked for. All-in, the typical cost was about 217 dollars a month. That is a business, and it helps to see it as one.
If you are getting a GLP-1 online, and plenty of good people are, a real evaluation looks about like this. A real clinic asks about your history, not just your goal weight. It wants some actual numbers, ideally recent labs. It screens for the things that make these drugs a bad idea for certain people, eating disorders included. You talk to a real person, and you get to confirm the order before anyone charges your card.
If none of that happened, and the drug was in your cart in five minutes, you did not see a doctor. You used a vending machine that happens to require a credit card.
I am not going to tell you to stop. I am on one of these myself. I am telling you to notice which one you are standing in front of.
Primary sources
- Chetty AK, Chen AS, Ross JS, Ramachandran R. “Online Prescribing of GLP-1 Receptor Agonists.” JAMA, published online July 6, 2026. doi:10.1001/jama.2026.9131. jamanetwork.com
- Banks A. “GLP-1 Receptor Agonists and Eating Disorders: Cause for Concern.” N Engl J Med. 2026;394(17):1665-1667. doi:10.1056/NEJMp2600300
- Related DadStrengthDaily cornerstone: Who’s Really Writing Your Online Prescription?
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, and prostate or cancer screening.