
I got the two-dose Shingrix series at 52 because my wife had shingles a couple of years ago and it was, as she would put it, the worst pain she has ever been in. The rash settled within a few weeks. The nerve pain along the band where the rash had been took months to fade. She is not a complainer. The whole thing reset my opinion of the vaccine from “something to consider when I’m 60” to “find a pharmacy this weekend.”
That decision now looks better in retrospect than it did at the time. In the eighteen months since, the evidence that Shingrix does more than just prevent the rash has piled up faster than almost any other intervention in adult medicine.
The original case for Shingrix is still the case
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
Shingles is a reactivation of the varicella-zoster virus, the same virus that gave you chickenpox at age four. After the chickenpox cleared, the virus stayed dormant in your nervous system for the rest of your life. Decades later it can wake up, follow a single nerve back to the skin, and produce the rash my wife had. The rash heals. The nerve damage is the bigger problem.
About one in ten people who get shingles end up with postherpetic neuralgia, persistent nerve pain along the affected dermatome that can last months or years. A smaller subset get ocular shingles that can damage vision permanently. The CDC estimates one in three Americans will get shingles in their lifetime if not vaccinated.
Shingrix is roughly 90% effective at preventing the rash and the worst complications, and the protection lasts at least seven years on the strongest data we have so far. The current FDA approval is for adults 50 and older, plus immunocompromised adults 19 and older. That has not changed.
What has changed is everything we are learning about the off-target benefits.
The dementia signal
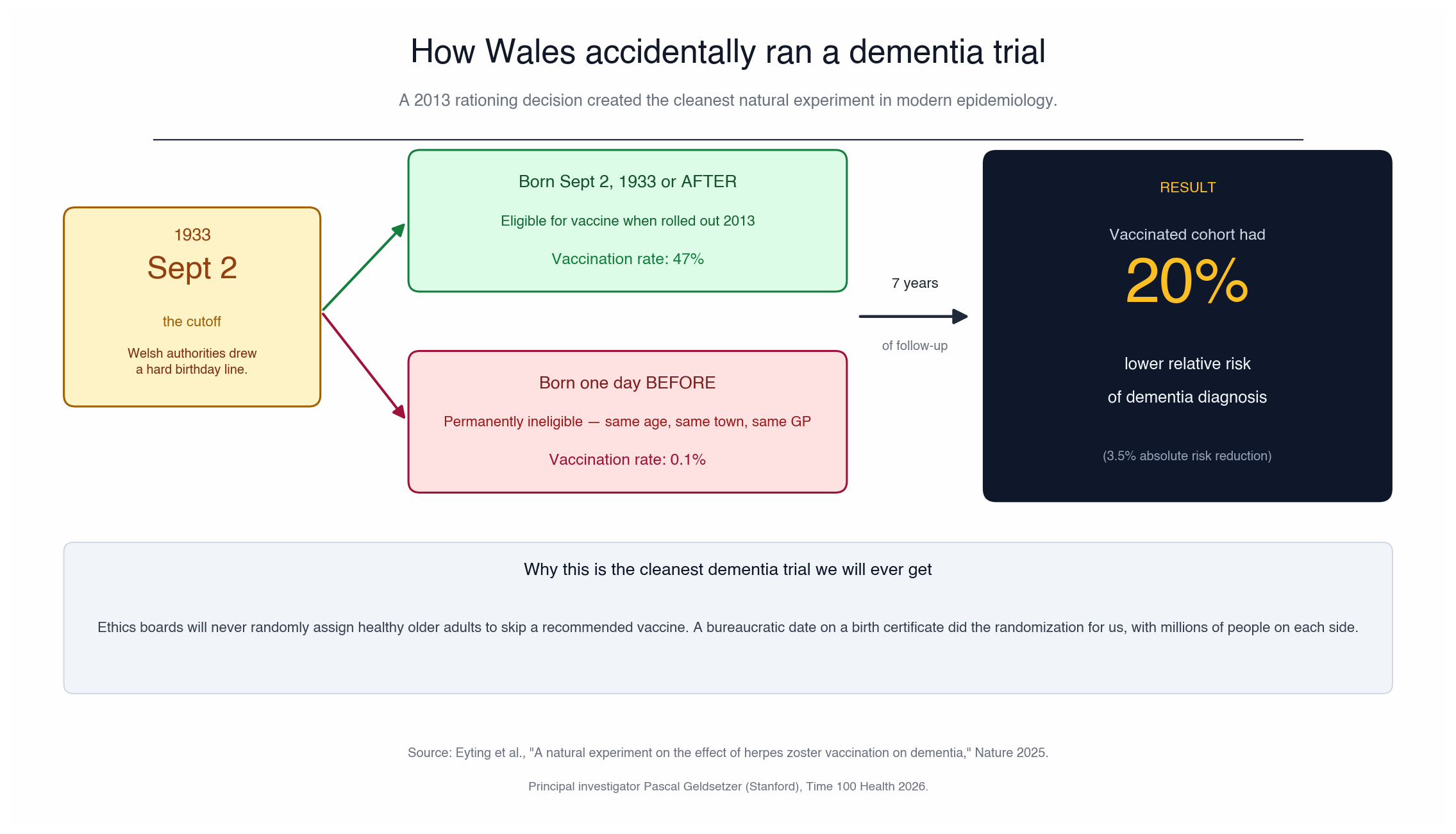
The flagship paper landed in Nature in May 2025. Pascal Geldsetzer, a Stanford epidemiologist named to the Time 100 Health 2026 list for this work, looked at a quirk in how Wales rolled out the shingles vaccine in 2013. To ration the supply, Welsh health authorities had drawn a hard birthday cutoff. Anyone born on or after September 2, 1933 was eligible. Anyone born one day earlier was permanently locked out.
That is a near-perfect natural experiment. People born a week before versus a week after that date are otherwise identical. The only thing that differs is vaccine access.
After seven years of follow-up, the vaccinated had a 20% relative reduction in new dementia diagnoses, a 3.5 percentage point absolute drop. About 47% of the eligible cohort actually took the vaccine, so the 20% number is the instrumental-variable estimate scaled to people who actually got the dose, not the smaller intent-to-treat effect on eligibility alone.
A 20% relative risk reduction on dementia, from a vaccine already sitting in pharmacy fridges everywhere, is the kind of finding that should have led every health desk for a month. It mostly did not.
A follow-up in Cell in December 2025 by the same team looked at how the vaccine worked at different stages of dementia. The protective signal extended both backward (reducing new mild cognitive impairment diagnoses, the transitional stage before dementia) and forward (reducing mortality in people who already had a dementia diagnosis at vaccination).
The obvious objection was that the Wales study used Zostavax, the old live-attenuated vaccine, which has been retired and is no longer available. The US standard since 2017 has been Shingrix, a recombinant subunit vaccine. A US replication published earlier in 2026 followed adults 65 and older who got Shingrix and found a comparable reduction in dementia diagnoses. The new vaccine looks at least as protective as the old one on this endpoint.
The proposed mechanism is straightforward. The varicella-zoster virus chronically irritates the immune system in ways that drive neuroinflammation, contribute to amyloid accumulation, and damage cerebrovascular tissue. Preventing the reactivations reduces that chronic inflammatory load. It would explain both Alzheimer’s-type and vascular dementia signals showing up in the same dataset.
The cardiovascular signal
The other major finding came out of South Korea in 2025, and like the Wales dementia paper it studied the old live Zostavax vaccine, not Shingrix. Lee et al., publishing in the European Heart Journal, followed 1.27 million Korean adults aged 50 and older using propensity-score overlap weighting to match vaccinated and unvaccinated populations over a median of six years. The vaccinated had a 23% lower risk of cardiovascular events overall, 26% lower heart failure, and 26% lower major adverse cardiovascular events. The signal lasted out to eight years.
A March 2026 meta-analysis pooling nine studies showed the same direction with more conservative magnitudes.
A direct cardiovascular trial of Shingrix has not been run. The proposed mechanism, preventing the shingles event itself, would apply equally to either vaccine, since Shingrix prevents the rash at least as well as Zostavax did. But the specific cardiovascular magnitudes here come from live-vaccine cohorts and should not be read as Shingrix-confirmed.
The healthy-user-bias objection is real and worth flagging. People who voluntarily get a non-mandatory vaccine tend to also see their doctor more often, take medications consistently, and have generally better health behaviors. Some of the apparent benefit is almost certainly that.
But the Korean study has a tell against pure selection effects. The cardiovascular benefit was strongest in the unhealthiest subgroups, smokers and sedentary patients especially. That is the opposite of what you would expect if vaccination was just a proxy for being a generally healthy person. If the whole thing were selection bias, you would expect the cleanest signal in the people with the cleanest lives.
The mechanism is even simpler than the dementia one. Active shingles itself substantially raises stroke and heart-attack risk in the first one to three months after the rash. Preventing the index event prevents those downstream cardiac events.
What about people under 50?
The 50+ recommendation is the official guidance, and the evidence does not yet support pushing it earlier in healthy adults. Shingles incidence under 50 in immunocompetent people is low. The dementia and cardiovascular trial populations were all 50+. Definitely talk to your doctor as you would need a prescription under 50, i.e. you can’t just walk in at a drugstore.
If you are immunocompromised, the recommendation is age 19 and older, and that one should not be negotiable. Otherwise, wait until your 50th birthday and then act on it the way you would act on a colonoscopy. It is on the must-do list.
Practical notes
Shingrix is the vaccine you will feel. Sore arm, fatigue, headache, sometimes a low-grade fever. About one in six people have a reaction strong enough to interfere with the next day. The standard advice from anyone who has actually scheduled the shot for patients is to book it Friday afternoon so the worst of it lands on a Saturday morning, not at work.
If you got the old Zostavax years ago, the CDC currently recommends getting the two-dose Shingrix course anyway. Shingrix is more protective against the rash and the off-target benefits look at least as good.
The total cost is around $200 per dose without insurance. Most adult Medicare Part D plans now cover it at zero out-of-pocket after the 2022 Inflation Reduction Act changes. Insurance pre-65 varies, so check before you go in.
What I would do at 53
I already did it. I got Shingrix because I watched my wife suffer, not because of dementia or cardiovascular data that did not exist yet. The fact that those off-target benefits have accrued so quickly in the eighteen months since is essentially a free upgrade I did not pay for. The shingles avoidance was the point. Everything else is bonus.
If you are 50 and have not had the shots, the case has gotten substantially stronger since the last time you might have thought about it. Talk to your doctor or just get it at Walgreens/CVS like I did. The day-after sore arm is a tiny price compared to what my wife went through, and an even smaller price compared to what shingles can do to your nerves, your vision, your brain, and apparently your heart.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.