
The trials that quietly turned blood-sugar medicines into heart, kidney, and weight drugs.
I take a diabetes drug. I have never had diabetes.
That sounds like a mistake, and not long ago it would have been one. The drug is tirzepatide, sold as Mounjaro for diabetes and Zepbound for weight. I take it for weight. My last A1C, the three-month average of my blood sugar, came back at 4.9, which is normal. So why is a guy with normal blood sugar on a diabetes drug at all?
Because these drugs changed jobs.
A reader put me up to this. After I wrote up the new cholesterol pill and the ladder of drugs that lower LDL, he asked for the same map for blood sugar, and I realized I had been carrying the same wrong idea he did. I thought these were all just different ways to push a number down. A week in the trials fixed that.
Before I go further: I am on tirzepatide, and I own a little Eli Lilly stock, so I have a foot in this. None of what follows is medical advice. It is a map, and the person to read it with is your doctor, not me.
The old way was chasing one number
For a long time, treating type 2 diabetes meant chasing the A1C down. Start on metformin. When the number drifted back up, add a sulfonylurea. When that stopped holding, start insulin. Every rung got picked mainly for how far it drove the number down, on the theory that a lower number meant a healthier patient.
It was not wrong. Years of high blood sugar wreck small blood vessels, and getting it down protects eyes, nerves, and kidneys. But the system treated the reading as the finish line. Hit your target, you win.
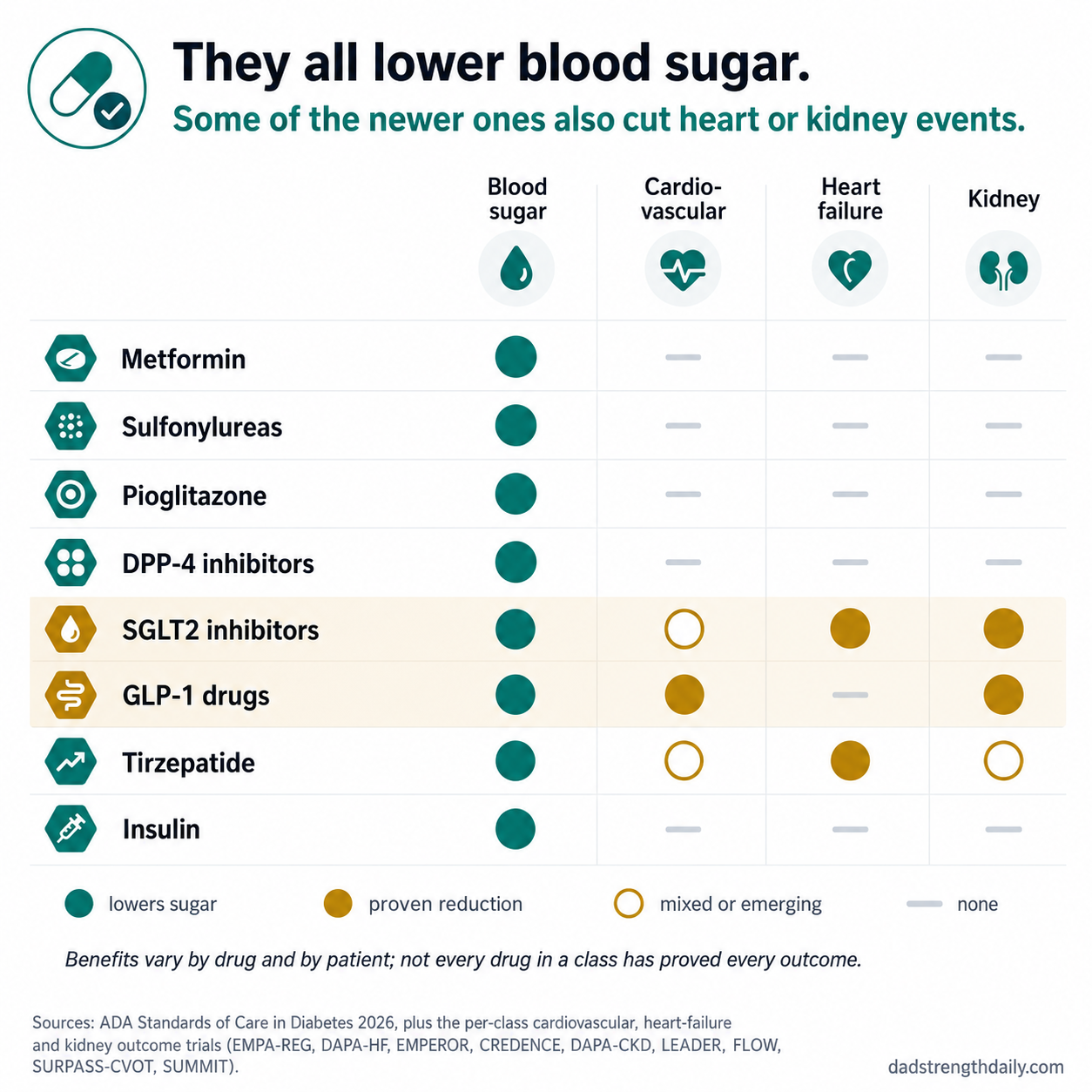
The lineup
Here is the roster, roughly in the order the drugs showed up.
Metformin is the cheap foundation, and for most people it still comes first, though as you will see that is no longer automatic. It is generic, a few dollars a month, knocks about a point off your A1C, and it will not drive your sugar too low on its own. It has been around since before I was born and it still earns its spot.
After that come the old add-ons. Sulfonylureas, like glipizide, work by flogging the pancreas to dump insulin whether the moment calls for it or not, which is why they cause low blood sugar and put weight on. Pioglitazone makes you more sensitive to insulin but brings fluid retention. Doctors still reach for both, because they are cheap, they genuinely lower the number, and for some patients that is enough. They have just slid down the pecking order for reasons about to become obvious.
Then the mild modern pills. DPP-4 inhibitors, the common one being sitagliptin, sold as Januvia, nudge your own gut hormones up a little. Gentle, weight-neutral, not very strong, and easy to add.
And then the two classes that rewrote the category.
SGLT2 inhibitors, the ones ending in “-flozin,” make you spill extra sugar out in your urine. On paper that is a modest way to lower blood sugar. What they actually turned out to do is the reason half this piece exists. GLP-1 drugs, semaglutide and its cousins, are the ones you have heard about at every party for two years, strong on sugar and strong on weight. Tirzepatide, the one I take, is a weekly shot that hits two gut-hormone targets instead of one and is among the most powerful glucose-lowering drugs available, lowering A1C by more than two points in some trials.
Insulin is the oldest and most powerful glucose-lowering tool in the room. In type 2 diabetes it is usually added when the other drugs are not enough, though very high blood sugar or real symptoms can make it necessary sooner.
The accident that changed everything
In 2008, after an older diabetes drug got tangled up in a heart-risk scare, the FDA started demanding that every new diabetes medication prove it did not raise the risk of heart attacks and strokes. It was a safety exercise. Run a big, long heart-outcomes trial, show you do no harm, get to market.
One of those safety trials went sideways in the best way. In 2015, EMPA-REG OUTCOME tested the SGLT2 drug empagliflozin in people with type 2 diabetes and existing heart disease. It was built to rule out harm, not to find benefit, and it found a big one anyway. Cardiovascular deaths fell from 5.9 percent of patients to 3.7 percent, a bit more than a third lower. Put another way, treating about 45 of these high-risk patients for roughly three years prevented one cardiovascular death; for death from any cause, the number was about 39. It also cut heart-failure hospitalizations by about a third. The drug that makes you pee out sugar was suddenly a heart drug.
After that the dam broke. GLP-1 shots like liraglutide and semaglutide ran their own heart trials and cut cardiovascular events too. The SGLT2 drugs went on to protect failing kidneys, slowing the damage by roughly a quarter, and to keep people out of the hospital for heart failure, in trials that included people who did not even have diabetes. The size of the benefit varies by drug and by how sick the patients were, but the pattern held. I had filed all of these under “blood sugar.” The trials made me refile them under “heart and kidney.”
How the choice works now
Picking a type 2 diabetes drug in 2026 looks nothing like climbing the old ladder. The current ADA guidelines do not start everyone on metformin and work up by the number. They start by asking what else is wrong.
Heart failure points toward an SGLT2 drug, because it keeps people out of the hospital. Kidney disease, much the same, sometimes with a GLP-1 instead. Existing heart disease, obesity, or substantial weight-management goals may point toward a GLP-1 drug or tirzepatide. This is a simplified map, and the real decision also turns on kidney function, side effects, and cost. But the spine of it is new. You can end up on one of these based on your heart and kidney risk, sometimes before your exact A1C even comes up, and sometimes instead of the cheap old pills that move the number just as well. Metformin is not automatically first anymore. That is a genuinely recent change, and the guidelines only caught up to it over the last few years.
I have watched this movie before
If that shape feels familiar, it is because I walked you through the same thing with cholesterol, where lipid medicine spent years picking drugs by how far they pushed LDL down, then reorganized around the ones proven to prevent heart attacks. The lab value still matters, but what I care about, for my own heart, is whether the drug prevents the event the number was warning me about. Blood sugar is learning that lesson about a decade behind.
The money, and the part that just changed
The cost map has its own kink, and the numbers here are a mid-2026 snapshot, because this corner moves fast. The old generics are almost free, a few dollars a month for metformin and the older pills. And in April 2026 the FDA approved the first generic versions of dapagliflozin, one of those organ-protecting SGLT2 drugs. It now runs about eight dollars a month at Cost Plus, against roughly six hundred for the brand. One of the category’s outcome-proven drugs just got cheap.
Coverage is the catch. The GLP-1 shots and tirzepatide are the pricey corner, still near a thousand a month at list, and plans often pay for them when the label says diabetes but not when it says weight, which is a different fight. To get around that, Lilly now offers direct self-pay vials and KwikPens, with regular prices running from about $299 to $699 a month depending on dose. So the cheapest options in the category are some of the most protective, and the priciest are the ones you may have to argue your insurance into. I do not fully trust the self-pay prices to stay this low, but for now they are real.
Back to me
So, me. I take tirzepatide for weight, not sugar. My A1C is a normal 4.9, and I am not managing a disease I do not have. I can take it because it was tested and approved separately for weight, sold under the name Zepbound, which is its own story apart from the heart-and-kidney one I just told. But the two rhyme. The same molecules turned out to do so much more than lower glucose that “diabetes drug” stopped describing them well.
If you actually have type 2 diabetes, here is the part worth carrying into your next appointment. The question is not only what your number is. It is why you are on this particular drug, given your heart, your kidneys, and your weight. A1C still matters. It just does not answer that by itself.
A caveat before you go: those trial results are averages in specific high-risk groups, not guarantees for any one person, and the best drug depends on the rest of your health. This is a map, not medical advice, so talk to your own doctor before you change anything.
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.