
I told you in my cholesterol explainer that an oral version of the most powerful cholesterol drugs was coming. As of today, it is here. Whether you need it is a different question.
Back when I wrote my plain-English guide to reading your cholesterol panel, I ran through the six families of drugs that lower cholesterol and got to one of the most powerful classes, the PCSK9 inhibitors. They cut your LDL by more than half, and until now every one of them was an injection. I mentioned, almost in passing, that an oral version called enlicitide was in late trials and might land in a year or two.
It landed today. The FDA approved it as Lipfendra, the first PCSK9 inhibitor you swallow instead of inject. That is a genuine milestone. It is also being written up everywhere this afternoon as if it changes everything, so let me do the thing this blog exists to do and tell you what it actually is, what it costs, how it stacks up against the shots, and who it is really for.
What got approved
Lipfendra, generic name enlicitide, is a once-daily tablet. In the two trials it was approved on, it lowered LDL cholesterol by about 56 percent against placebo in the main study and about 59 percent in patients with the inherited form of high cholesterol. It also dropped ApoB, the count of cholesterol-carrying particles that can sharpen your risk picture when it disagrees with your LDL number, by roughly half. Almost everyone in those trials was already taking a statin. The approved label is broad, an add-on to diet and exercise for adults with high cholesterol including the inherited kind, and it does not require you to fail anything first. In real life, though, clinicians will usually reach for it after a statin and often ezetimibe, since that is who the trials studied, and insurers will likely gate it behind those cheaper drugs. Someone who genuinely cannot tolerate statins is a separate case.
Those numbers put it right in the range of the injectable PCSK9 drugs. For the first time, that level of LDL lowering comes in a pill. Here is where it sits on the same ladder I drew in the explainer.
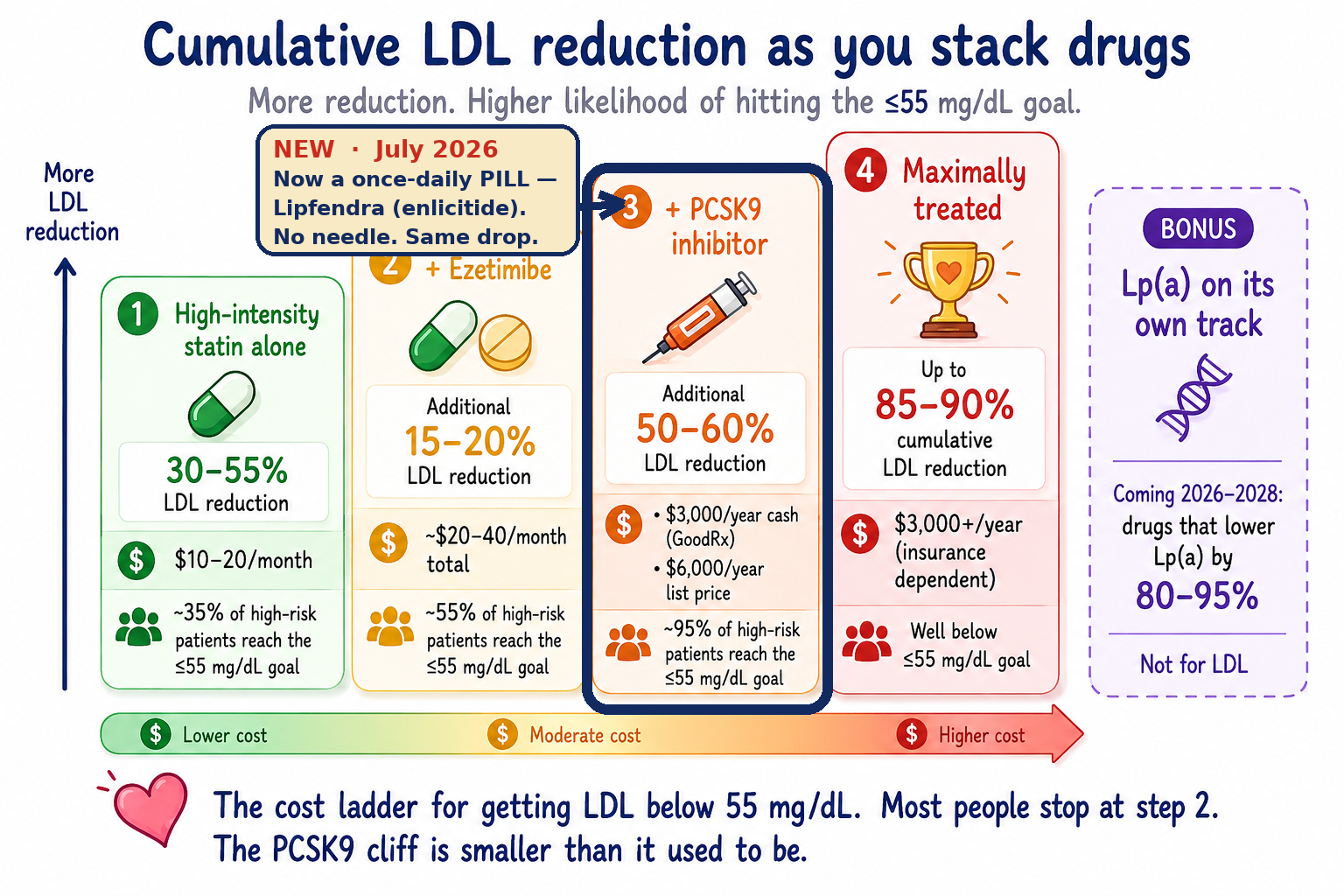
Pill versus shot
The two original PCSK9 shots are evolocumab, sold as Repatha, and alirocumab, sold as Praluent. You inject those yourself under the skin every two to four weeks, and they live in your refrigerator. A newer one, inclisiran, sold as Leqvio, is a shot a nurse gives you in the office twice a year after the first couple of doses. Lipfendra is a tablet you take every morning.
On lowering LDL, they all land in the same range. Lipfendra cut it about 56 percent against placebo in its trial. The most-studied injectable, evolocumab, ran about 59 percent in the FOURIER trial; alirocumab landed around 55 percent in ODYSSEY OUTCOMES; and twice-a-year inclisiran comes in near 50 percent. Those numbers come from separate trials in different patients, not a head-to-head, so read them as the same ballpark rather than a ranking. The takeaway holds: the pill is not more powerful than the shot. It matches the shot, minus the needle and the injection training. For the person who has quietly told their doctor no to an injection, that is the whole story.
The convenience has a small catch. You take Lipfendra on an empty stomach in the morning, then wait at least thirty minutes before eating or drinking anything other than water, black coffee, or plain tea. Its prescribing information says it can be taken with other medications, and Merck’s own interaction study found no meaningful effect between Lipfendra and the oral Wegovy pill that a lot of you are already taking. The wrinkle is that oral semaglutide has its own strict morning ritual, empty stomach and a small sip of water, so if you are on both, ask a pharmacist or your prescriber how to line them up rather than guessing. A pill is not automatically effortless. It is just a different routine than a shot you take twice a year.
The outcomes trial is still running
Lipfendra was approved on how far it lowers LDL, not on a finished trial showing it prevents heart attacks. Merck says as much: it is not yet known whether the pill cuts cardiovascular events. Its outcomes trial, CORALreef Outcomes, enrolled more than fourteen thousand people and has an estimated primary-completion date in late 2029, so the definitive cardiovascular evidence is still several years away.
I would keep that in perspective. Lowering LDL is about the most reliable surrogate in cardiology. Decades of genetics and trials point the same way, that you drop LDL and events fall roughly in proportion, more or less regardless of how you drop it. Lipfendra hits the very same target as Repatha and Praluent, the injectable PCSK9 drugs that already have completed outcomes trials. That prior evidence makes a heart benefit for Lipfendra biologically plausible. It just has not been demonstrated for this drug yet, and it will be a few years before it is. For someone with established heart disease, especially after a prior heart attack, the completed outcomes data still gives Repatha and Praluent an edge for now.
The safety picture from the trials was reassuring, close to placebo overall, with somewhat more diarrhea (7 percent versus 2 percent) and dizziness (9 percent versus 4 percent) in the familial-hypercholesterolemia study.
What it costs, and whether your insurance will play along
The list price is about $10.50 a day, roughly $3,800 a year. List price is almost never what anyone actually pays, though, so here is how the pill lands next to the injectable PCSK9 drugs. Fair warning that Lipfendra is brand new, its launch timing and coverage are not yet clear, so treat its row as a placeholder.
| Drug | List | Self-pay | With card |
|---|---|---|---|
| Lipfendra (daily pill) | ~$315/mo | n/a yet | n/a yet |
| Repatha (shot) | ~$490/mo | $239/mo | from $25/mo |
| Praluent (shot) | ~$490/mo | $392/mo | from $50/mo |
| Leqvio (2×/yr) | ~$3,590/dose | n/a | from $0 |
That table leaves a lot out. The cash programs bypass insurance, so they may not count toward your deductible, and the coupon prices vanish the moment you are on Medicare or Medicaid. What is fair to say is that the pill’s list price undercuts the old injectable stickers, but what you actually pay still comes down to your plan.
And I would keep those expectations low. Whenever the pill reaches pharmacies, every lesson from the last decade of PCSK9 drugs says the insurer will make you climb the cheap rungs first. Expect prior authorization, a documented LDL still above target, and proof you already tried a statin and ezetimibe. When the injectable versions launched, one analysis of more than forty-five thousand patients found fewer than half ever got approved, and a third of the approved prescriptions were never even filled once the copay showed up. Coverage has improved a lot since then. But a lower sticker price does not mean a low copay, and it does not mean an easy yes.
Who this is actually for
I can see this mattering for a handful of people. Someone with the inherited form of high cholesterol who is nowhere near goal even on a statin. Someone with documented statin intolerance, for whom a clinician might consider Lipfendra without a statin behind it. The cholesterol specialist Tom Dayspring, who I wrote about, is exactly that case: he can take neither a statin nor ezetimibe, so the two cheap rungs of the ladder are simply gone for him, and a drug like this becomes especially relevant. And plenty of people just will not inject themselves, and now they do not have to. This class of drug left all of them out for a decade because it only came with a needle.
I am not one of them, and this is where I will be honest about my own panel. My LDL is 56 and my ApoB is 59, and I got there without a statin at all, through losing the weight, a GLP-1, and a cheap generic called ezetimibe. The whole story is here. My doctor and I were comfortable with that at my risk level. It is not a universal swap, and someone starting from higher risk than mine may still need a statin as the primary treatment. But I am the guy this pill is not for, and my hunch is that a lot of you are too. Many people who need to lower their cholesterol can reach their target on a statin and ezetimibe, two generics that together run about a dollar a day. That is a lot of money to answer a question most of us do not have.
None of that makes the approval small. It is a real advance, and for the people in those three groups it is the best news this drug class has had in years. It just is not the news most of us need. Measure yourself against the ladder before you reach for the top rung, and if you have not read the full cholesterol panel guide yet, start there and get your ApoB checked.
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.