
Tom Dayspring taught a generation of doctors how to lower LDL. He can’t tolerate the cheap drugs that do it. When he needed the expensive one, his insurer decided his numbers were too good to cover.
I take a cholesterol drug that costs about twenty dollars a month, and it works. One of the most influential cholesterol educators alive cannot take it, or the statin it is usually paired with, and when he needed the expensive drug instead, his insurer told him he was not sick enough.
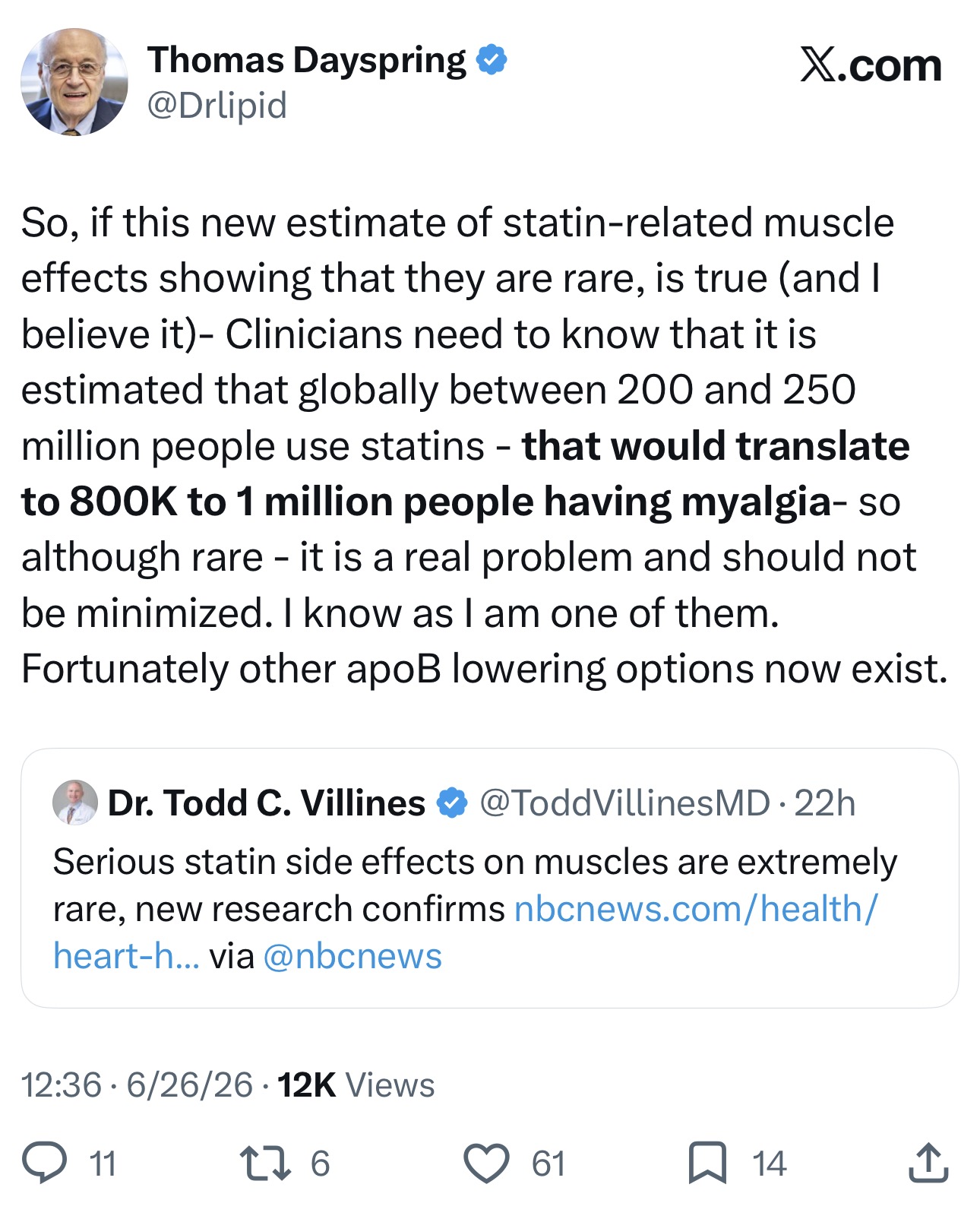
Last week a new analysis confirmed that serious muscle damage from statins is genuinely rare. That finding matters, because fear of side effects keeps a lot of people off a drug that would help them. Tom Dayspring shared it and agreed with it. Then he added a detail about himself: “I am one of them.” Not the common statin complaint, the vague aches that often turn out to be the nocebo effect rather than the pill. The real kind, the kind that shows up in the urine.
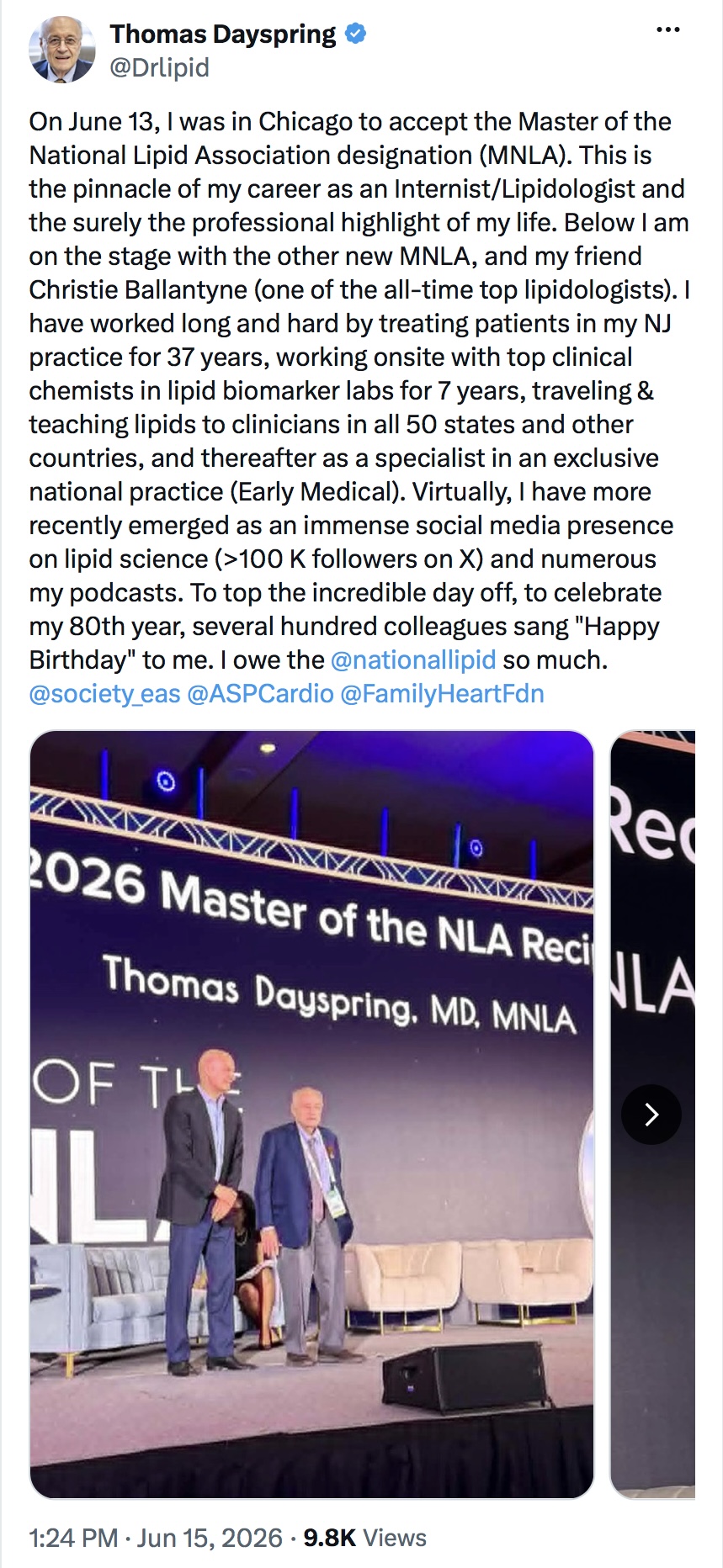
If you have learned anything about cholesterol from a podcast, the explanation probably traces back to Dayspring. He is an internist and clinical-lipidology educator, Peter Attia’s go-to expert on lipids, and this month he turned eighty and was named a Master of the National Lipid Association, the highest honor his field gives. He has taught a generation of doctors how to drive LDL down. He cannot take the drugs that do it.
For almost everyone, lowering LDL starts with a statin. Dayspring’s body treats statins as a threat. He has said they gave him myoglobinuria, muscle protein leaking into the urine, the early edge of the kind of muscle breakdown that can wreck the kidneys and land you in the hospital. The standard backup is ezetimibe, the same cheap generic I take without thinking about it. Unusually, it gives him severe muscle pain too. So both of the first-line drugs are out for him. For a long stretch he had no good option at all.
He needs the treatment as much as anyone does. Fifteen years ago his coronary calcium score came back over three hundred. A score above three hundred is commonly treated as high risk, the kind of number that means real plaque is already built into the artery walls, not a theoretical future risk. He has documented coronary disease. He is exactly the patient the aggressive-treatment guidelines are written for. He just cannot get there the usual way.
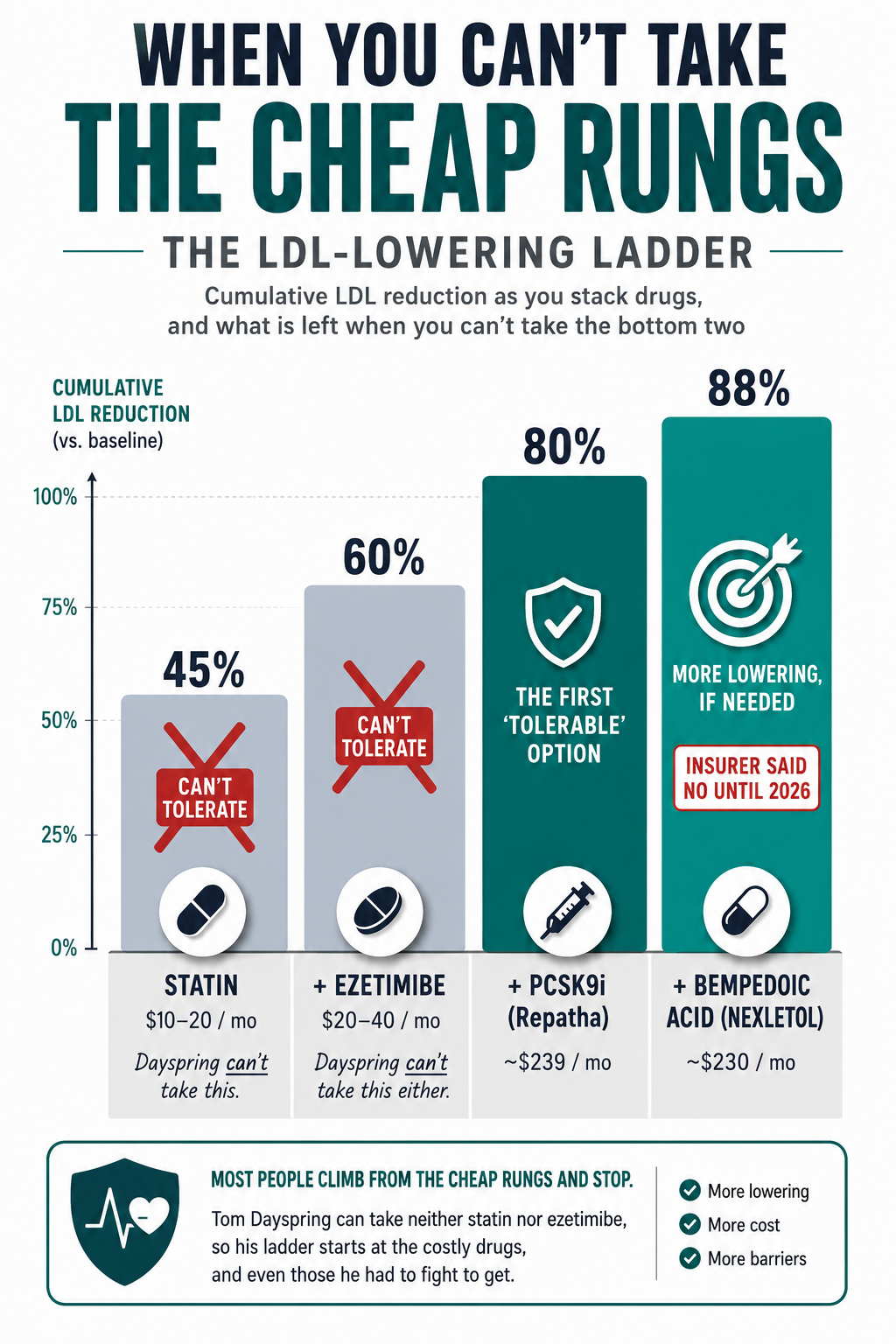
When PCSK9 inhibitors arrived about a decade ago, one of them, evolocumab, sold as Repatha, became his entire regimen. These are injectable drugs that lower LDL sharply, and they sit near the top of the cost ladder. For many people who reach goal on a cheap statin and ezetimibe, the extra benefit does not justify the price, which is why insurers and doctors reserve them. For Dayspring it runs the other way. The Repatha is not an upgrade sitting on a cheap foundation. With the statin and ezetimibe gone, it is the foundation. On that drug alone, his ApoB, the count of the particles that actually drive plaque, falls into a range most people reach only on a full statin regimen.
PCSK9 inhibitors launched at very high prices, so insurers built gates around them: prior authorization, the rules about who qualifies. Reserve the expensive drug for the people who most need it. Reasonable enough, until you watch what the gate does to someone like Dayspring.
When he first needed one, his plan refused to pay, because he had not had a heart attack yet. He had the plaque, the high particle count, the documented disease, and the clinical judgment of one of the best lipid doctors alive. Not enough. As he recounted on The Proof with Simon Hill, they wanted him to have his first heart attack, and then they would cover it, if he survived.
Dayspring tells it himself on The Proof (Ep 253, March 2023). The clip opens at 1:12; the line about needing a heart attack first lands at 1:13:15.
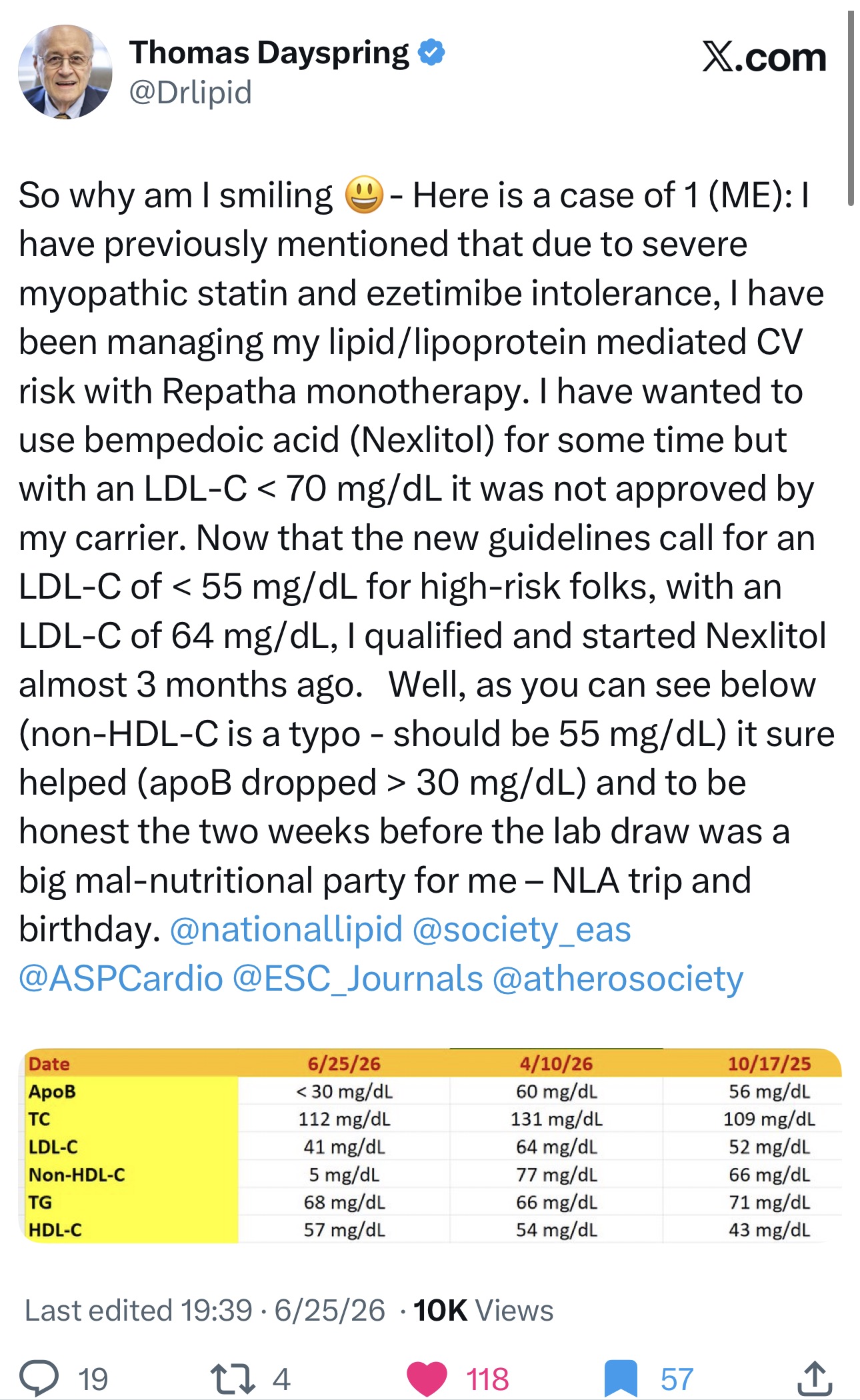
He won that fight in the end, and a PCSK9 inhibitor has carried his risk ever since. Then it happened again this spring. Even on Repatha his LDL sat at 64, above the stricter goal his coronary disease called for, so he wanted to add bempedoic acid, an oral drug that lowers cholesterol without acting on muscle and one of the few a statin-intolerant patient can actually take. His insurer said no, because his LDL was already under seventy. His numbers were too good. He only qualified months later, when a new 2026 cholesterol guideline lowered the LDL goal for very-high-risk patients to fifty-five, and his LDL of 64 flipped from too good to not good enough. His body had not changed. A line in a guideline had. He posted the whole sequence on X, lab panel and all.
The rules have a specific blind spot. To get the expensive drugs approved, most plans require that you first try and fail a statin and ezetimibe. Insurers call it step therapy, and for many average-risk patients, the logic is understandable. But Dayspring failing a statin does not look like a lab value that would not move. It looks like muscle protein in his urine. Many forms do have a box for statin intolerance. The problem is what it takes to tick it: documented muscle injury, enzyme levels many times normal, several different statins tried and failed, the very experiments his body cannot safely run.
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
If you are fifty and looking at your own panel, the standard advice still applies. A statin and a little ezetimibe get most people to goal, me included, and you should not let anyone sell you a three-thousand-dollar-a-year drug you do not need. The exception is worth knowing, because it might be you. Real statin intolerance is rare, but it is real, and it is not the same thing as the nocebo effect, where the symptoms can feel completely real but, in blinded trials, often show up on placebo too. The people who genuinely cannot take statins are a small group who keep getting waved off as part of a much larger one. If you are in it, you are not asking for an upgrade. You are asking for your only treatment, from a system that can read your good numbers as a reason to refuse.
What helps is documentation. Ask your clinician whether ApoB and Lp(a), an inherited risk marker, would sharpen your real risk beyond the standard LDL number. If you are told you do not qualify because your numbers are not bad enough, that is a coverage rule talking, not a doctor: ask for the denial in writing so you can appeal, and consider a second opinion. The cash prices have also fallen: Amgen now sells Repatha directly to cash-paying patients for around two hundred forty dollars a month, down from list prices that once ran into five figures a year. That cash route is for people paying out of pocket, not those billing insurance or on Medicare, but it is a fallback for when the coverage fight drags.
Both fights, he eventually won. He had the knowledge, the persistence, and a specialist’s vocabulary to argue with, and he still had to wait for a committee to move a number before his own plan would agree. He is eighty, he has documented coronary disease, and he wrote the lectures on how to treat it. If that is the fight for the man who trained the field, picture the patient with none of those advantages, holding a denial letter and no idea it can be appealed.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.