
I take a daily lipid-lowering pill. I think most adults over 50 should look hard at whether they need to as well. Statins work. Ezetimibe works. Repatha works. The problem is that almost none of them work if you forget to take them. About half of patients prescribed lipid drugs drop them within a year. The lifetime-of-adherence problem is one of the reasons heart disease is still the number-one killer in the United States.
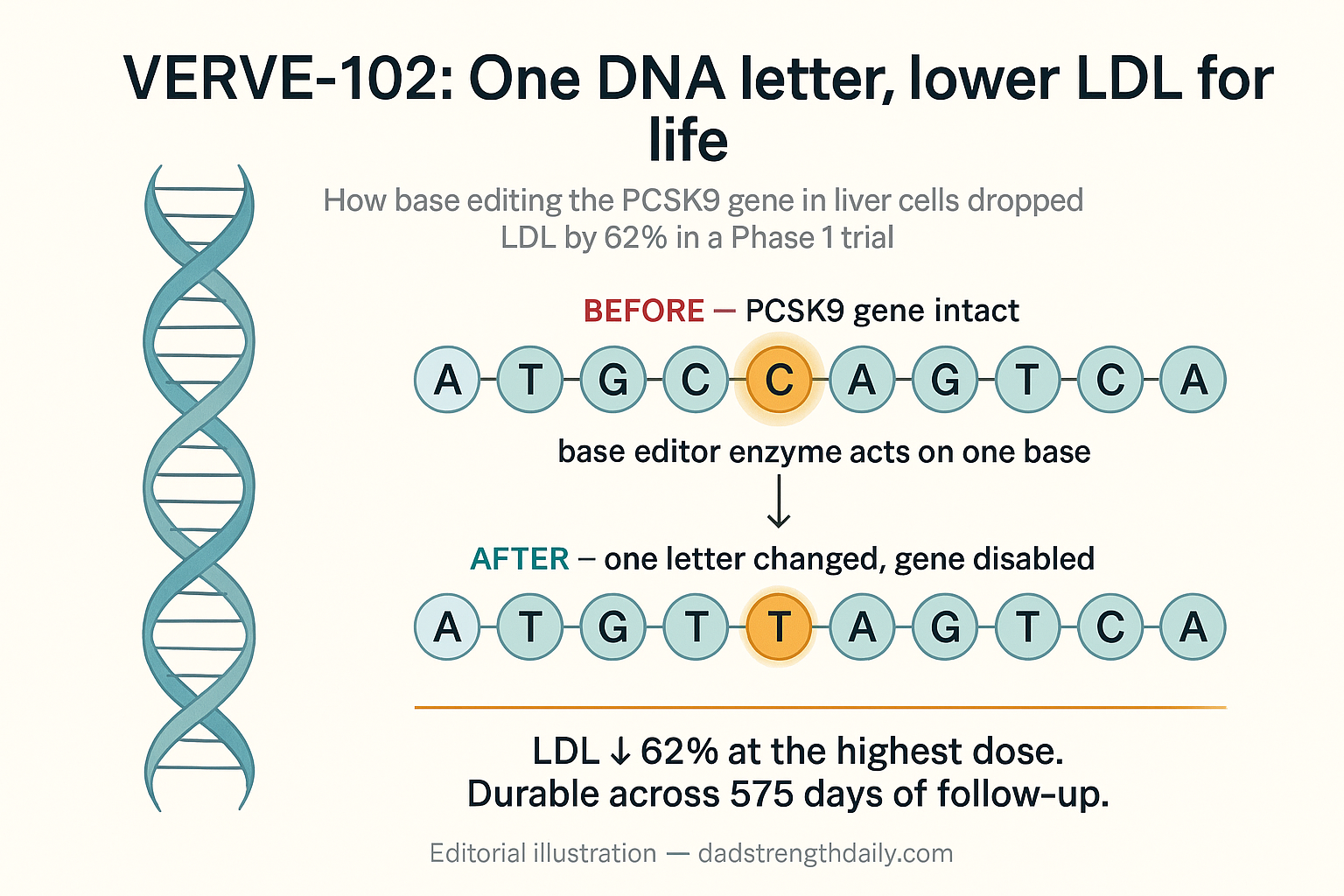
Eli Lilly just published Phase 1 data on a gene-editing therapy called VERVE-102 that proposes a different bargain. One infusion, LDL drops by 62 percent at the highest dose, and the effect appears permanent because the change is to your DNA. The data were published today in the New England Journal of Medicine and presented at the European Atherosclerosis Society meeting in Athens. STAT covered it here.
This is the strongest early evidence yet for a “one and done” approach to LDL lowering. It is also a permanent change to your DNA. Both halves of that sentence are pretty insane.
What VERVE-102 actually does
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
To understand VERVE-102 it helps to know where PCSK9 sits in the cholesterol-lowering landscape. PCSK9 is a protein your liver produces that breaks down LDL receptors on the surface of your liver cells. Fewer LDL receptors means less LDL gets pulled out of your bloodstream and into the liver for disposal. The various cholesterol drugs all increase LDL receptor activity, but they do it through different routes. Statins inhibit cholesterol synthesis in the liver, which prompts the liver to upregulate its LDL receptors to compensate. Ezetimibe blocks dietary cholesterol absorption in the gut, which produces the same downstream effect. Neither directly touches PCSK9. The PCSK9-targeted class is newer and works on the receptor-degradation side. Repatha and Praluent are monoclonal antibodies that bind PCSK9 in the bloodstream and neutralize it. Inclisiran is an RNAi drug that tells your liver cells to stop producing PCSK9 in the first place. All three of those work by holding the PCSK9 protein down while it tries to do its job.
VERVE-102 does something different. Instead of blocking the protein, it disables the gene that makes it. Specifically, it edits a single DNA letter in the PCSK9 gene inside your liver cells, which introduces a premature stop codon and prevents the protein from being produced. The technical name for this is base editing. Unlike traditional CRISPR, which cuts both strands of DNA and lets the cell repair the break (which can introduce errors), base editing chemically converts one DNA base to another without making a full cut. An adenine deaminase enzyme converts one base on one strand, and a modified Cas9 “nickase” makes a single nick on the opposite strand, which triggers the cell’s DNA repair machinery to finalize the edit. The result is a deliberate, targeted swap of one DNA letter for another, at one position in one gene, in one organ.
Because the edit is to your DNA, it is inherited by every new cell that descends from the edited liver cells. Every replacement liver cell carries the change. The PCSK9 protein is not produced. Your LDL receptors live longer. Your LDL drops. The therapy is delivered as an infusion into the bloodstream, packaged in lipid nanoparticles (the same delivery technology behind the mRNA Covid vaccines), with the nanoparticles preferentially taken up by liver cells.
It is a different kind of medicine than any cholesterol drug that came before.
The Phase 1 numbers
Thirty-five patients enrolled in the dose-escalation trial (called Heart-2), conducted in Australia, Canada, New Zealand, and the United Kingdom. The population was chosen for high cardiovascular risk: people with heterozygous familial hypercholesterolemia, or premature coronary artery disease (defined as disease onset at 55 or younger in men, 65 or younger in women). This is the population most likely to accept the risk-reward of an experimental gene therapy. “My LDL is mildly elevated” patients were not in the trial.
A critical detail that gets lost in some of the coverage: 91 percent of participants were already on a statin at baseline (71 percent on a high-intensity statin), and 43 percent were on ezetimibe. The 62 percent LDL reduction at the highest dose was on top of existing best-current-care therapy, not in place of it.
The seven patients on the highest 1.0 mg/kg dose saw an average LDL reduction of 62 percent and an even bigger 88 percent drop in PCSK9 protein itself. Median follow-up across all participants was about nine months, with 15 patients now followed for at least a year and the longest follow-up at 18 months. The effect appears durable across that window. Steven Nissen, the Cleveland Clinic cardiologist who has spent decades arguing for aggressive LDL lowering, told STAT the results “appear durable (likely permanent).”
There were no dose-limiting toxicities and no deaths. Treatment-related adverse events did occur in about a third of participants, mostly mild-to-moderate infusion reactions (20 percent of the cohort) that were managed during the four-hour intravenous infusion, with premedication. Three patients had transient liver enzyme elevations that resolved within a week. The single serious adverse event in the trial was a case of aspiration pneumonitis in a participant with a history of GERD and a hiatal hernia, which the site investigator assessed as unrelated to the drug. Verve had to shelve its first gene-editing candidate due to safety concerns, so the clean Phase 1 safety profile here is the second important finding, in addition to the cholesterol drop.
The unknowns are still substantial. Ninety days of follow-up on the highest dose is short. The trial enrolled fewer than a hundred patients. We do not yet have data on how the edit behaves over years or in patients with comorbidities. The Phase 2 trial that would test all that has slipped from its originally planned end-of-2025 start to end-of-2026.
The trade-off that has not been settled
When you stop taking a statin, your LDL goes back up within weeks. When you stop taking Repatha, your LDL goes back up within months. When you receive VERVE-102, the PCSK9 gene in your liver is changed for the rest of your life. You cannot undo it.
That is the trade-off Nissen flagged when STAT pressed him. “Gene editing is not for everybody,” he said. “It will take time and experience to determine who is best served by a one-time editing therapy.”
The case for VERVE-102 is strongest in people whose adherence to existing drugs is poor and whose cardiovascular risk is high. Sek Kathiresan, Verve’s co-founder and now a Lilly vice president, frames it in those terms. He told STAT that about half of patients drop their lipid medications within a year, which is the unmet need Verve is targeting. For a patient who carries familial hypercholesterolemia and has trouble staying on Repatha, a permanent edit is a different calculation than for a 55-year-old whose LDL is borderline and who is taking a daily Lipitor without much fuss.
The harder question, which Phase 1 data does not answer, is what happens if you make a mistake. If a patient turns out to have an off-target edit that causes a problem twenty years later, there is no antidote. The conventional drugs all have an off switch. Gene editing does not.
The technology may eventually get safer than it currently is. Other gene-editing companies are pursuing the same target with different editor architectures. Lilly itself is also developing edits aimed at Lp(a) and ANGPTL3, both of which I have or will be writing about. The category is becoming a horse race, with at least four serious entrants developing one-shot cardiovascular edits.
What this means if you are already on lipid meds
For most readers, this changes nothing about today. VERVE-102 is in Phase 1, will likely take another four to six years to reach approval if Phase 2 and Phase 3 land cleanly, and will probably be initially restricted to high-risk populations where the calculation clearly favors the edit. If your LDL is borderline and you are willing to take a daily statin or biweekly injection, this technology is not for you yet.
The piece that does change today is the framing of the long game. For decades, the assumption has been that cardiovascular prevention is a lifetime commitment to daily or biweekly medicine. Inclisiran moved that to twice a year. VERVE-102, if it proves out, moves it to once. The 2026 ACC/AHA cholesterol guideline that pushed the LDL target below 55 mg/dL for high-risk patients is going to look more achievable when achieving it does not require fifty years of pill-taking.
For my own situation, I am on daily ezetimibe and not in the high-risk genetic-mutation population. I would not be a candidate for VERVE-102 today even if it were approved. But I am paying attention. I would much rather hear, at 65, that one good infusion solves LDL problems for the rest of life than keeping up with daily pills. If the Phase 2 and Phase 3 trials hold up, the question I would actually be asking my doctor by 2032 is not “do I want this” but “is my risk profile high enough to be in the first wave.”
The catch, again, is that the change is permanent. That is the bargain. For the patients in this Phase 1 trial, it is the right bargain. For everyone else, the answer is “watch closely. The calculation is going to change.”
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.