
The categories didn’t move. A risk calculator did, and that quiet swap explains most of the noise.
I take a blood pressure pill every morning. Telmisartan, low dose, because my mother had high blood pressure and mine crept up enough that my doctor and I decided not to wait around. I keep a cuff on the kitchen counter and I actually use it. So when the headlines said the blood pressure guidelines had “changed again,” with men supposedly pushed out of treatment and women pushed in, I went and read what actually changed.
The short version: the numbers that define high blood pressure did not move at all. Not one of them. What changed is a piece of math that happens behind the curtain, in a calculator most people never see. And once you understand that calculator, most of the panic turns out to be aimed at the wrong thing.
The part everyone is getting wrong
Here is the thing the loudest posts keep missing. The categories are exactly the same as they were in 2017.
| Category | Reading | What it means |
|---|---|---|
| Normal | Under 120/80 | Nothing to treat. Keep it there. |
| Elevated | 120 to 129, and under 80 | Not a diagnosis, but a nudge. Lifestyle, no pills yet. |
| Stage 1 | 130 to 139, or 80 to 89 | The gray zone. This is where the decision lives. |
| Stage 2 | 140/90 or higher | High enough that medication is usually the answer. |
That “130 is now high” shift, the one that reclassified millions of people overnight, happened back in 2017, and it stuck. (I walked through what each of those category numbers actually means in an earlier piece.) The 2025 update left those lines alone.
So when someone tells you the new guidelines mean “more women are considered hypertensive now,” they have it wrong. The categories did not move, so the diagnosis did not move either. What changed is a narrower question: among people already sitting in that Stage 1 gray zone, who should actually start a pill. That is a treatment question, not a diagnosis question. A guy at 132/84 is Stage 1 under both the old rules and the new ones. The only thing in play is whether his risk number says pill now or lifestyle first.
The one thing that actually changed
To decide whether a Stage 1 patient needs medication, a doctor estimates your odds of a heart attack or stroke over the next ten years. If the risk is high enough, you treat. If it isn’t, you start with lifestyle and recheck.
The 2025 guideline changed the tool that produces that estimate. The old one was called the Pooled Cohort Equations. The new one is called PREVENT, and in the big head-to-head comparisons it tends to score people about half as high as the old calculator did.
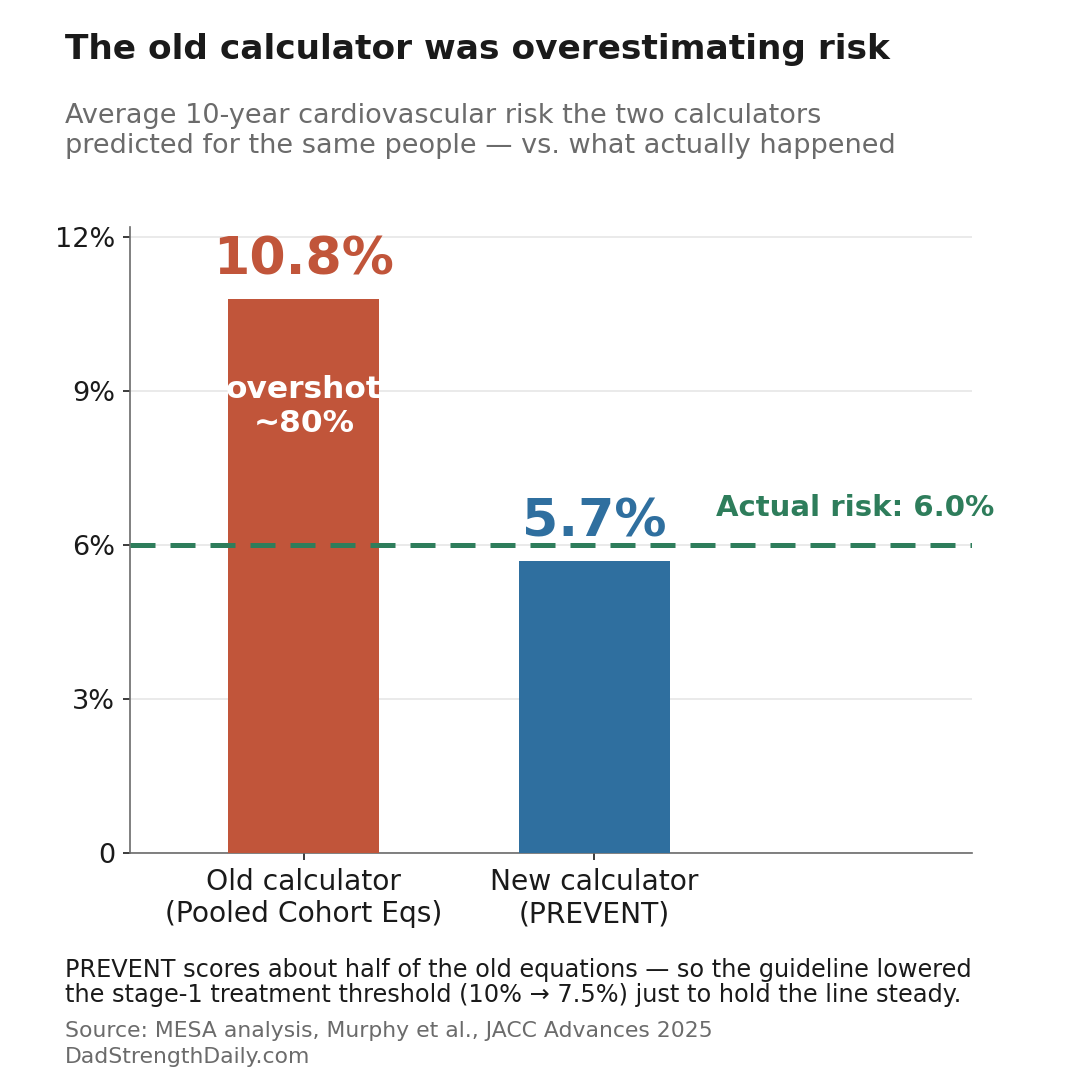
It sounds like a scandal until you see why. The old calculator ran on decades-old data and badly overshot. A 2025 analysis in the journal JACC Advances tested both tools against the long-running MESA heart study, where researchers had tracked real people for ten years. The old equations predicted an average risk of 10.8 percent. PREVENT predicted 5.7 percent. What actually happened was 6.0 percent. The old tool overestimated risk by about 80 percent. The new one tracked the observed risk much more closely.
PREVENT is also just a better-built tool. It drops race as an input, a change many clinicians and researchers had pushed for. Race is a rough social category, not something that moves blood pressure on its own, and baking it into the math mostly baked in old inequities. In its place PREVENT leans on things that actually move your heart risk, like your weight and your kidney function (the eGFR number on your lab work). Stuff the old model waved past. It even folds in heart failure, not just heart attacks and strokes, which matters more the older you get.
Why lowering the bar barely changed anything
Here is where it gets counterintuitive. Swap in a calculator that scores everyone lower, keep the old treatment cutoff, and you would suddenly drop a huge number of people below the line and pull them off their medication. A 2024 analysis in JAMA estimated that keeping the old threshold with the new calculator would have meant roughly 107,000 additional heart attacks and strokes. Nobody wanted that.
So the guideline lowered the treatment threshold at the same time, from a 10 percent risk down to 7.5 percent. That was not an expansion. It was a counterweight. A lower cutoff pulls more people in. A lower-scoring calculator pushes people back out. The two moves mostly cancel.
And the real-world numbers say exactly that. When the health-record group Epic Research ran both guidelines across 1.7 million adults with Stage 1 hypertension, the share eligible for medication went from 45.2 percent to 47.0 percent. A move of 1.8 percentage points. That still touches real people at the margins, but as a shake-up it barely registers.
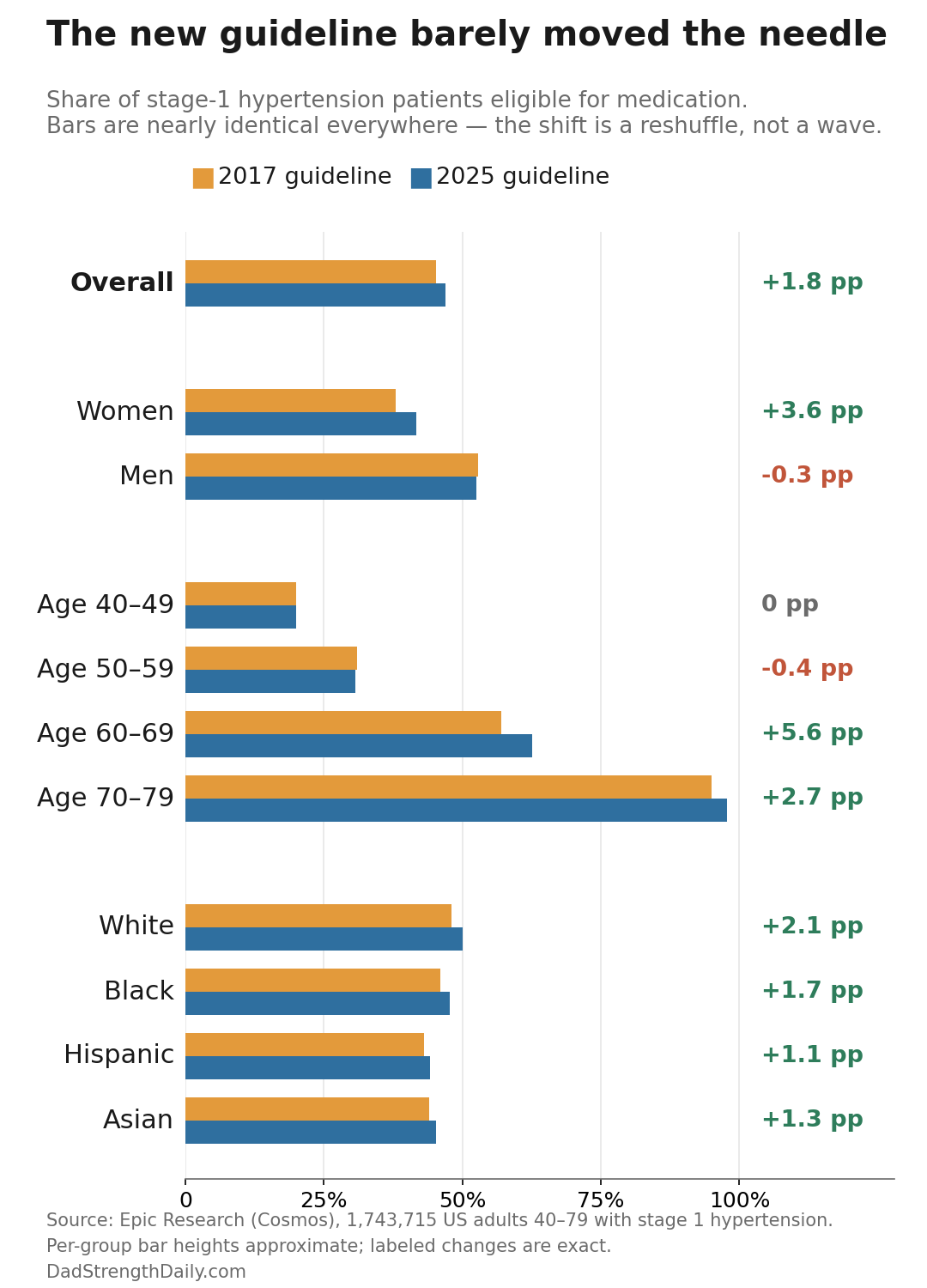
What did happen is a small reshuffle. Adults in their sixties gained the most, because that is where the more accurate math had the most room to work, and women gained a few points. As for the “men are being pushed out” storyline: men as a group dropped by three tenths of one percentage point. That is a rounding error, not a policy against your health. And the one group that did dip a little, by four tenths of a point, was people in their fifties of both sexes. That is not the same as “men in their fifties.” There is no such number in the data, even though that is how it keeps getting passed around.
What this actually means for you at 50
Strip away the calculator drama and the decision is simple. It comes down to which band your real number falls in, and by real I mean the average of several careful readings, ideally some taken at home, not one nervous measurement in a waiting room.
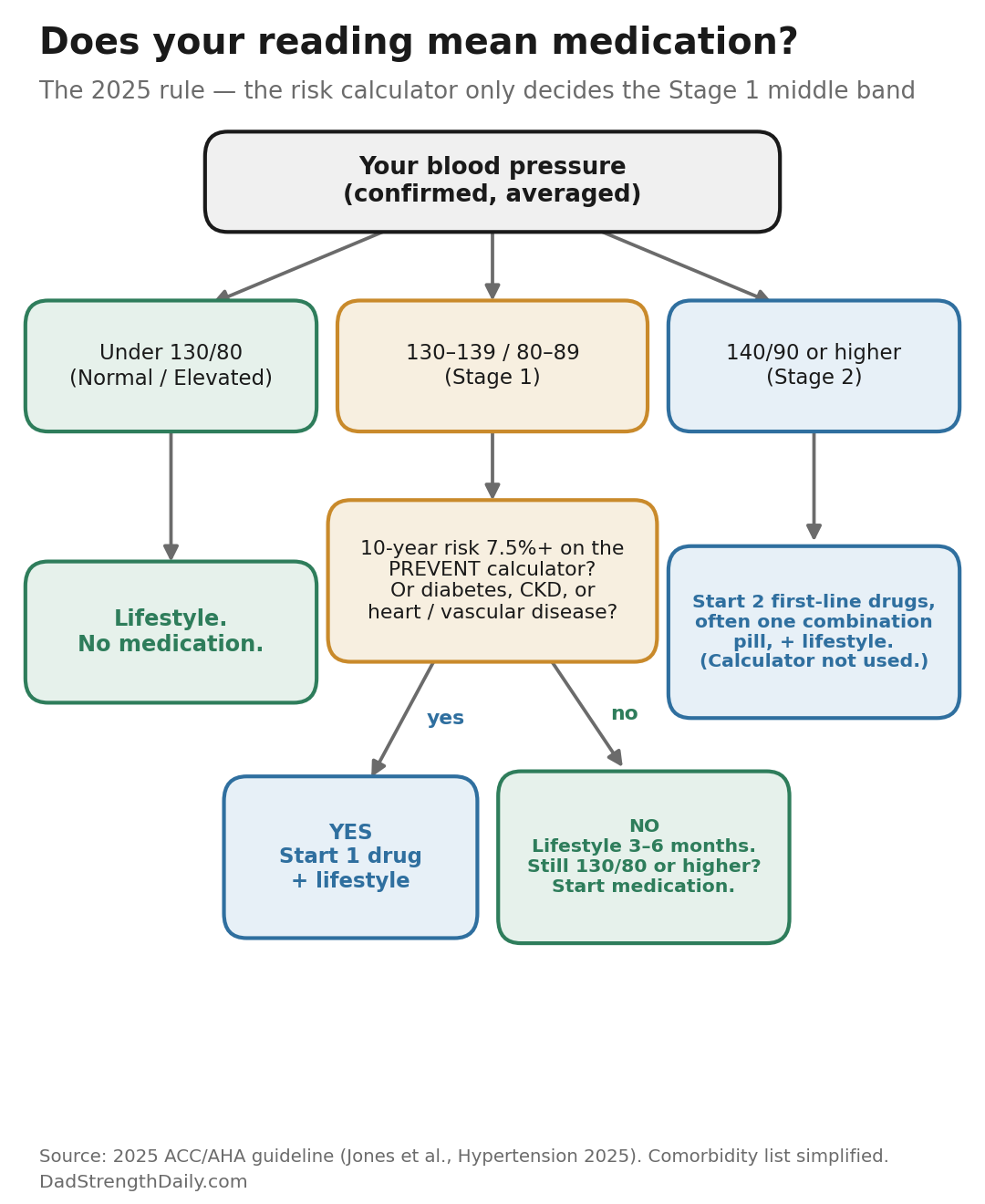
If your readings sit at 140/90 or higher, confirmed over more than one sitting, that is Stage 2, and medication is almost always part of the answer. The risk calculator barely enters the conversation at that level. The guideline continues to favor starting many Stage 2 patients on two first-line drugs at once, often combined into a single pill, because one drug alone rarely gets someone that high back to goal. Your doctor still weighs the usual things, like how far above goal you are, what else you have going on, and how you tolerate the drugs.
If you land in the Stage 1 gray zone, 130 to 139 over 80 to 89, it is a judgment call based on your risk. Your doctor runs the PREVENT number. If it clears 7.5 percent, or if you already have diabetes, kidney disease, or heart trouble you already know about, you start a pill along with lifestyle changes. If you are under that line and otherwise healthy, the guideline says to give lifestyle a real three to six month shot first, then recheck. If your average is still 130/80 or higher after that, the guideline says it is time to start medication.
And if you are under 130/80, you keep doing the boring things that got you there.
One last thing, and it is the part I would actually do. You can run your own PREVENT number before you ever sit down with your doctor. The American Heart Association put the calculator online for free. You plug in your blood pressure, cholesterol, weight, and a few other numbers, and it hands you a ten year and a thirty year estimate. It is only as good as the numbers you feed it, so if your cholesterol or kidney labs are a couple of years stale, treat the result as a conversation starter, not a verdict. Even so, walking into that appointment already knowing your number changes the conversation from “should I be worried” to “here is my number, what do we do about it.”
One warning before you go play with it: do not stop, start, or change a blood pressure medication based on a calculator alone. The number is there to sharpen the conversation with your doctor, not to replace it.
The honest read
This is a headline that sounds like a shake-up and is really a quiet accuracy fix. The guideline writers swapped an outdated calculator for a much more accurate one, then adjusted the treatment line so the change in the tool did not accidentally yank people off their meds or pile new ones on. The net effect on who actually gets treated is tiny. What you are left with is a better tool that finally accounts for things like weight and kidney function, and the same advice that was true last year.
Know your real number. Take it more than once, sitting quietly, not right after coffee or a fight with the printer. If you are high, take it seriously and talk treatment with your doctor. Untreated pressure is one of the most preventable ways to lose years you did not have to lose, and no calculator was ever going to change that.
Get the next one in your inbox
I write about longevity, training, and preventive health weekly, without the guru worship. Free, no spam, unsubscribe whenever.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, and prostate or cancer screening.