
I take the drug that just won on weight loss.
A network meta-analysis landed in The BMJ this week, pooling 262 randomized trials and nearly 100,000 people to rank the obesity drugs against each other. It was publicly funded, not paid for by any drugmaker, though several of its authors consult for the companies whose drugs it ranks. Tirzepatide, the shot I inject every week under the brand name Zepbound, came out on top for pure weight loss. But the drug that strips off the most weight is not the drug with the strongest evidence for the outcomes I actually care about, staying alive and out of the hospital. Those turned out to be two different medicines.
I am staying on tirzepatide anyway. It wins on weight but does not yet have equally strong obesity-specific outcome evidence, and that tension is worth walking through.
Disclosure: I take Zepbound and own Lilly shares. Full disclosure at the end.
What 262 trials actually measured
A network meta-analysis is a way to compare drugs that were mostly never tested against each other directly. A few head-to-head trials do exist, like SURMOUNT-5, which put tirzepatide against semaglutide for obesity in 2025. But across the full field of 19 drugs, most of the direct match-ups have never been run, so the math stitches the separate trials, each tested against placebo or lifestyle changes, into one ranking. This is the biggest such analysis yet done on obesity drugs: 19 medicines, follow-up from a few months to more than three years, graded for how trustworthy each finding is.
One detail made me feel seen. The median age across all those trials was 49. The median starting BMI was about 35. That is not a room full of 25-year-olds chasing a beach body. That is my demographic, sitting in the exact spot where the weight has consequences.
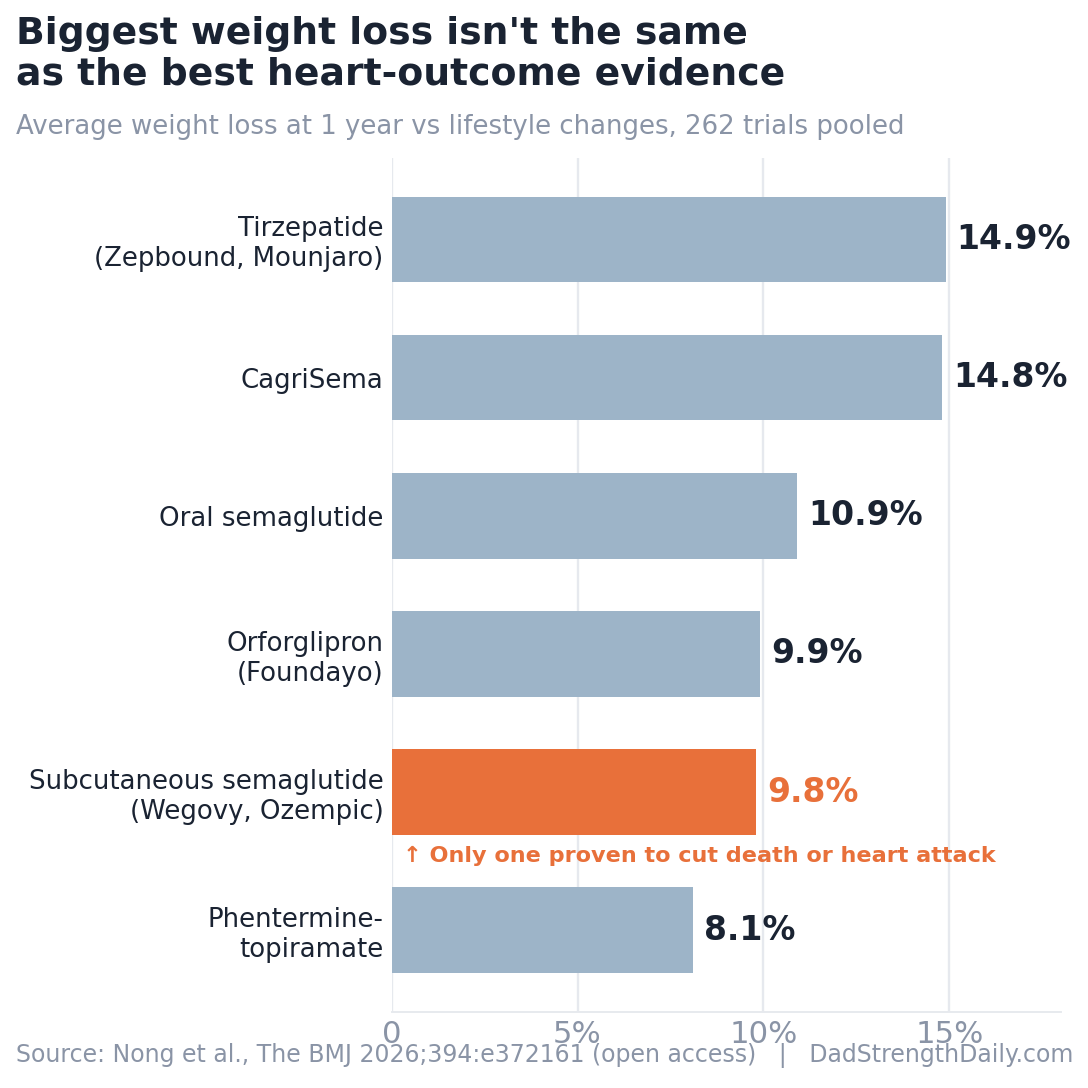
For weight loss at one year, measured against lifestyle changes alone, the top of the table looks like this:
| Drug | Weight loss at 1 year | Proven to cut death or heart attack? |
|---|---|---|
| Tirzepatide (Zepbound, Mounjaro) | 14.9% | Not in an obesity trial yet |
| CagriSema | 14.8% | Not yet |
| Oral semaglutide | 10.9% | Not yet |
| Orforglipron (Foundayo) | 9.9% | Not yet |
| Subcutaneous semaglutide (Wegovy, Ozempic) | 9.8% | Yes, in people with heart disease |
| Phentermine-topiramate | 8.1% | Not yet |
Weight-loss figures versus lifestyle changes alone, moderate-to-high certainty. Source: Nong and colleagues, “Comparative effects of drugs for adults with overweight or obesity,” The BMJ 2026;394:e372161 (open access).
Tirzepatide at almost 15 percent is a genuinely big number. Roughly a third to a half of people on it or on CagriSema hit at least 20 percent weight loss inside a year, which the authors point out starts to approach what some bariatric surgeries deliver. The newer triple agonists like retatrutide may land even higher, but the evidence there is still thin, so the study rated it low-certainty and I am not counting it yet.
The number I care about more than the scale
Weight is a proxy. What I actually want is more years and fewer heart attacks. On that question the ranking flips.
Subcutaneous semaglutide, the molecule sold as Wegovy for weight and Ozempic for diabetes, was the only drug in the whole analysis with high-certainty evidence that it lowers all-cause death (risk ratio 0.81, about 19 percent lower, 95 percent confidence interval 0.72 to 0.93) and heart attacks (0.72, about 28 percent lower, 0.61 to 0.85). That evidence rests almost entirely on one kind of study: cardiovascular-outcome trials run in people who already had heart disease. The pivotal one, SELECT, enrolled 17,604 adults who had established cardiovascular disease and overweight or obesity but no diabetes, and over about three years the rate of heart attack, stroke, or cardiovascular death fell to 6.5 percent on semaglutide from 8.0 percent on placebo. Those are relative reductions in a high-risk group, not a promise that a healthy 40-year-old on the same shot buys extra decades.
Tirzepatide did not clear that same bar, but not because it has no outcome data at all. In SURPASS-CVOT, a trial of more than 13,000 people with type 2 diabetes and heart disease, tirzepatide matched dulaglutide, an older GLP-1 that already lowers cardiovascular risk, for heart attack, stroke, and cardiovascular death (hazard ratio 0.92, 0.83 to 1.01). It held even, but it did not win. What tirzepatide is still missing is a placebo-controlled trial in people with obesity, rather than diabetes, that counts deaths and heart attacks the way SELECT did for semaglutide. That trial is running and has not reported. So the honest gap is not “no evidence,” it is “no obesity outcome trial yet.”
There is one place tirzepatide has its own hard-outcome data. In SUMMIT, a trial of 731 people who had both heart failure with a preserved ejection fraction and obesity, tirzepatide cut a composite of cardiovascular death and worsening heart failure by about a third (hazard ratio 0.62). Read the fine print, though. The benefit came almost entirely from fewer worsening-heart-failure events, not from fewer deaths, and it was shown in that specific group, not in everyone who takes the drug. The BMJ analysis credits both semaglutide and tirzepatide with lowering heart-failure risk, but tirzepatide’s share of that rests heavily on this one narrow trial.
The muscle I am trying not to give back
Every one of these drugs takes some lean mass along with the fat. Tirzepatide took the most, about 8 percent, measured on DEXA scans, which capture lean mass overall rather than skeletal muscle alone. That headline scared a lot of people, me included, until you read the other half of the same sentence: it also stripped the most fat, about 26 percent. Far more of what comes off is fat than lean tissue. The ratio is on your side, not against you.
The fix is not a different injection. It is the boring thing. When I put myself in a DEXA scanner to see what I was actually losing, the answer tracked with the guidelines the BMJ authors quote at the end of their paper: resistance training and enough protein are sensible ways to protect lean mass, though nothing guarantees you keep all of it. I wrote more about why that muscle-loss fear is usually overblown if you actually lift. The drug is not an excuse to skip the gym. It is the reason to finally go.
What none of the shots fixed
Two findings kept me honest about the whole category.
First, quality of life. On the generic quality-of-life scales the trials used, none of the drugs crossed the study’s threshold for a clinically important average improvement at one year, across 43 trials and 45,000 people. That does not mean nobody felt better. It means the trials did not prove a large enough average change on those instruments. Read it as a limit of what those questionnaires captured, not proof that the weight loss does nothing for you. It is still a fair splash of cold water on the idea that a lower number on the scale automatically rewrites how you feel.
Second, it only works while you are on it. A 2026 BMJ review that pooled 37 trials found people regain weight at about 0.4 kilograms a month after stopping, roughly a pound, and the cardiometabolic gains, the better blood pressure and blood sugar, drift back toward baseline within about a year and a half. Real-world data says roughly half of patients quit within the first year, usually because of nausea, other gut trouble, or fatigue. This is a long-term relationship with a medication, not a summer fling. I did not fully understand that when I started.
What this means in practice
If your goal is the most weight lost. Tirzepatide and CagriSema lead.
If you already have heart disease. Subcutaneous semaglutide has the clearest evidence for fewer heart attacks and deaths.
If you have heart failure with a preserved ejection fraction plus obesity. Tirzepatide has real trial evidence, but only for that group.
Whatever you pick. Access, tolerability, dose, your other conditions, and your doctor’s read matter as much as the ranking does.
Why I am not switching
If I had established cardiovascular disease and were choosing mainly on outcome data, semaglutide would be the easy call today. It has the mortality numbers. Nothing else does.
I am staying on tirzepatide for reasons that are specific to me. It gives me the biggest weight reduction. It also has the heart-failure data I mentioned, which I pay attention to given my own cardiovascular history, though that trial was in a narrow group and is a conversation for my doctor rather than something I map straight onto my own risk. And switching off something that is already working has its own downside. That is a shared decision I made with my doctor, which is exactly the frame the study lands on. It ranks the drugs, then refuses to crown one, because the right answer depends on whether you are optimizing for weight, for your heart, for cost, or for what your insurance will actually cover.
Two questions I had quietly let blur together turn out to be separate: which drug takes off the most weight, and which drug has the strongest evidence so far for helping people avoid the outcomes that matter. Right now they have different answers. Worth knowing before you pick.
Disclosure: I take tirzepatide (Zepbound). I also own shares of Eli Lilly, which makes tirzepatide, orforglipron, and retatrutide. I have no position in Novo Nordisk. None of this is medical advice. Talk to your own doctor before starting, stopping, or switching any of these medications.
Get the next one in your inbox
I cover the latest GLP-1 trials and access changes weekly. Free, no spam, unsubscribe whenever.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, and prostate or cancer screening.