
The training habit it left me with was the real thing.
I never exercised. Not a sport I let lapse, not a gym membership I stopped using. For about thirty years of adult life, exercise was a thing other people did while I worked. Then at 50 I started losing weight on a GLP-1, and one warning followed me everywhere I read: a big share of what you drop on these drugs isn’t fat, it’s muscle, and the only thing that protects it is lifting weights. That scared me. So I bought a pair of dumbbells, I started force-feeding myself protein, and I got to work.
Here is the twist. That fear turned out to be badly overblown. The muscle-loss panic I’d been sold was mostly a misread scan and a lot of people with something to sell. But by the time I understood that, lifting had quietly become the best decision I’d made in a decade. I want to walk you through both halves, because the reasons to train at 50 turned out to have almost nothing to do with the thing that scared me into it.
One note before we go further. I’m not a doctor, and nothing here is medical advice or a reason to start, stop, or change a medication on your own. This is one engineer’s read of the research and his own experience, and the drug decisions belong between you and your physician.
The headline that scared me into the gym
When you start reading about GLP-1 drugs, the muscle warning is impossible to miss. The number that launched it came out of the semaglutide STEP 1 trial, where a body-composition substudy found that close to 40 percent of the weight people lost showed up as lean mass on the scan (Wilding et al., 2021). Forty percent. Say that to a middle-aged man who is already losing sleep about getting old and frail, and you have his full attention.
The framing around that number was apocalyptic. You were going to melt. You’d end up “skinny fat,” lighter on the scale but weaker and softer than before. Ozempic was eating your muscle. Some of the early concern came from people I respected, including Peter Attia, who flagged lean-mass loss on scans in his own practice. When smart people you trust are worried, you get worried.
I did what a scientist-brained beginner does with a fright like that. I overcorrected. I decided that if the drug was going to strip muscle, I would out-train it and out-eat it. I hit protein like it was a second job, aiming well past what I’d ever eaten before. And I started lifting, badly and randomly at first, because the alternative in my head was wasting away. The whole story of how I fumbled my way from a corner of my home office to a real program is its own post. Fear got me started. I was training to defend against a threat.
Get the next one in your inbox
I cover the latest GLP-1 trials and access changes weekly. Free, no spam, unsubscribe whenever.
Even the scary scan showed a normal split
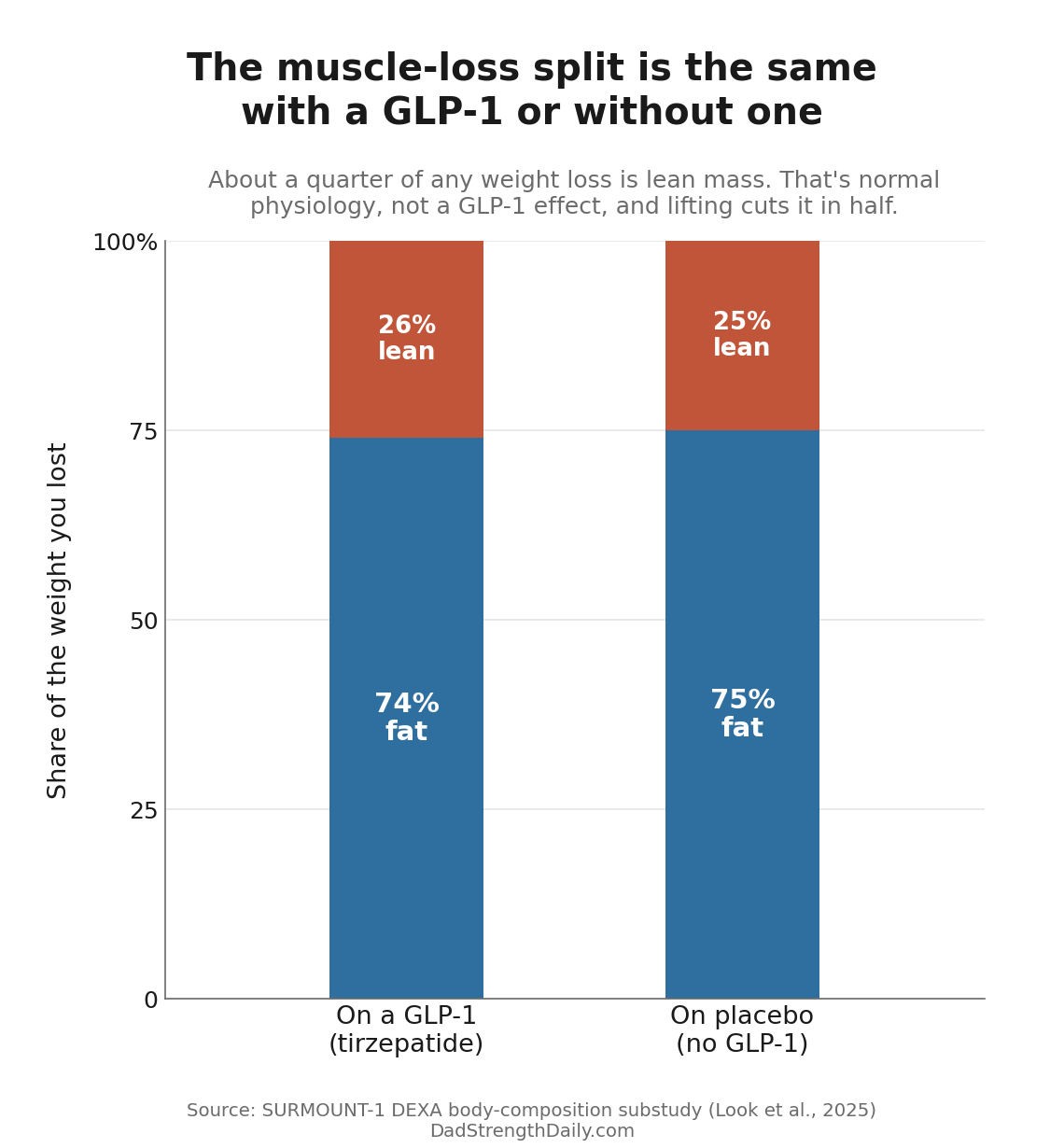
The misleading part was the missing context. Nobody ever put the GLP-1 number next to the obvious comparison, the same amount of weight lost without a drug.
Even measured on the same kind of DEXA scan that started the alarm, the share of weight that comes off as lean mass on a GLP-1 is ordinary. In the tirzepatide SURMOUNT-1 body-composition substudy, 26 percent of the weight people lost was lean mass, and in that same study, people in the placebo group who lost weight without any drug lost 25 percent of theirs as lean mass (Look et al., 2025). Same split. Diet and bariatric surgery land in the same neighborhood, roughly a fifth to a third of the weight lost. When one health system compared more than a thousand bariatric-surgery patients with about two thousand people on semaglutide or tirzepatide, surgery caused more total weight loss and more absolute muscle loss, but the share that came off as lean stayed in the same modest range for both (2026 cohort). No one has run the cleaner experiment of matching the exact pounds lost across methods, but the pattern keeps repeating: how much muscle you lose tracks how much weight you lose, not which method got you there. Losing some lean mass alongside the fat is just what human weight loss looks like, whether the cause is a salad or a syringe. STEP 1’s near-40 percent turned out to be on the high end, and larger, later studies came in lower. The honest read isn’t that the drug spares your muscle or that it eats it. It’s that losing some lean mass is what losing weight does, at about the rate any method of losing weight does it. And because the fat loss dwarfs it, the ratio of fat to lean mass improves either way. You come out leaner, not softer.
On top of that, the scan overstates even that muscle loss. A DEXA machine does not actually weigh your muscle. It measures bone and fat and drops everything else into a bucket it labels lean mass, most of which is water, glycogen, and your organs. Lose weight fast and you dump stored glycogen and the water bound to it, an enlarged fatty liver shrinks back toward normal, and the fat marbled inside your muscles burns off. The scan logs much of that as lean mass walking out the door, even though not all of it is the contractile muscle that actually moves you. So the true loss of the tissue you care about is smaller than that already-ordinary quarter.
If you take a forty-pound backpack off your shoulders, your legs no longer need as much muscle to haul you up the stairs, and shedding a little of it is a healthy adaptation, not a wound. Spencer Nadolsky, an obesity doctor who has dug into this, keeps making both points at once: the loss is about what you’d expect from any calorie deficit, and better imaging that separates real muscle from water and fat shows the scan numbers were overstated. Even the early worriers have landed somewhere calmer. Attia’s more recent take is that the loss is not beyond what the weight loss would predict, and that strength and physical function usually improve, not decline.
You’d also expect a frailty signal in the big trials if these drugs were quietly crippling people, and it isn’t there. In SELECT, a trial of more than 17,000 people on semaglutide, serious adverse events were actually lower than on placebo, about 33 percent versus 36 percent (Lincoff et al., 2023). And in the STEP trials, patient-reported physical functioning improved more on the drug than on placebo (STEP patient-reported outcomes, 2024), because unloading forty pounds of fat does more for how a body moves than a modest dip in muscle takes away.
The muscle you do lose is not chemical destiny. It’s the predictable result of eating very little and not asking your muscles to do anything. In the S-LITE trial, people who added an exercise program while holding a big weight loss preserved their lean mass and improved their fitness, while the group on the drug alone did not (Lundgren et al., 2021). Training plus enough protein doesn’t just slow the loss, it largely protects against it. The tool I’d bought out of fear was the actual answer, just to a much smaller problem than I’d been told.
The worry is real for one group. A sedentary eighty-five-year-old with almost no muscle reserve losing more of it deserves real attention to strength and protein, as do frailer patients generally. But that is not the fifty-year-old man the viral headlines were built for. For him, the whole thing resolves into something boring and doable.
What I’d actually do on a GLP-1
Lift two or three days a week, eat enough protein (roughly 1.6 grams per kilogram of your goal bodyweight), and keep a loose eye on your strength and how you move day to day. Be more careful, and lean on your doctor, if you’re older, frail, eating very little, or already low on muscle.
Where the muscle-loss fear actually comes from
If the science is this reassuring, why is your feed still full of Ozempic-is-eating-your-muscles content? Mostly it isn’t a conspiracy. It’s confusion. The people repeating the warning saw the scary 40 percent number, never saw the comparison that makes it ordinary, and passed it along in good faith. That’s the biggest source by far, and the most fixable: put the placebo bar next to the drug bar and the fear usually lets go.
Then there are the people working an angle. Fitness influencers and online coaches are the loudest, and the platforms pay them in clicks for it. “The shot is melting your muscle, here’s my twelve-week plan to save it” is a perfect pitch: the same boring advice, lift and eat protein, wrapped in urgency and sold at a price. Hiring a coach for accountability is money well spent, and I do exactly that. Being scared into a program by the person selling it is a different thing.
There’s a quieter, angrier version too. Some people did it the slow, hard way and seem to hold a grudge about there being an easier path, so a GLP-1 reads as cheating and muscle loss becomes the price you must be paying somewhere.
The commercial players are real, just not the loudest, only the most motivated. Drug companies are building muscle-preserving compounds to sell alongside GLP-1s; the maker of my own paid nearly two billion dollars for one. Men’s-health clinics and the peptide crowd upsell testosterone and injectables as mandatory protection. The supplement aisle repackages amino acids as “Ozempic defense.” None of it is the emergency it’s dressed up as.
I have nothing against the useful tools in that pile. Creatine is worth taking and cheap, and protein matters. But the fear doing the selling is the fear the data deflates. The most honest muscle-preservation plan on earth costs nothing but time: pick up heavy things a couple of times a week and eat enough protein.
The real reasons to train at 50 have nothing to do with Ozempic
The fear got me into the gym, then it evaporated, and I kept going, because somewhere in that first year the muscle-on-a-GLP-1 question turned out to be the least interesting reason to train. I’ve come to think of what you’re building at 50 as a physiological pension. Nothing you do in the gym pays off much tomorrow. It pays off at 75, in whether you can carry your own groceries and get up off the floor without a plan. And it applies to every man my age, GLP-1 or not.
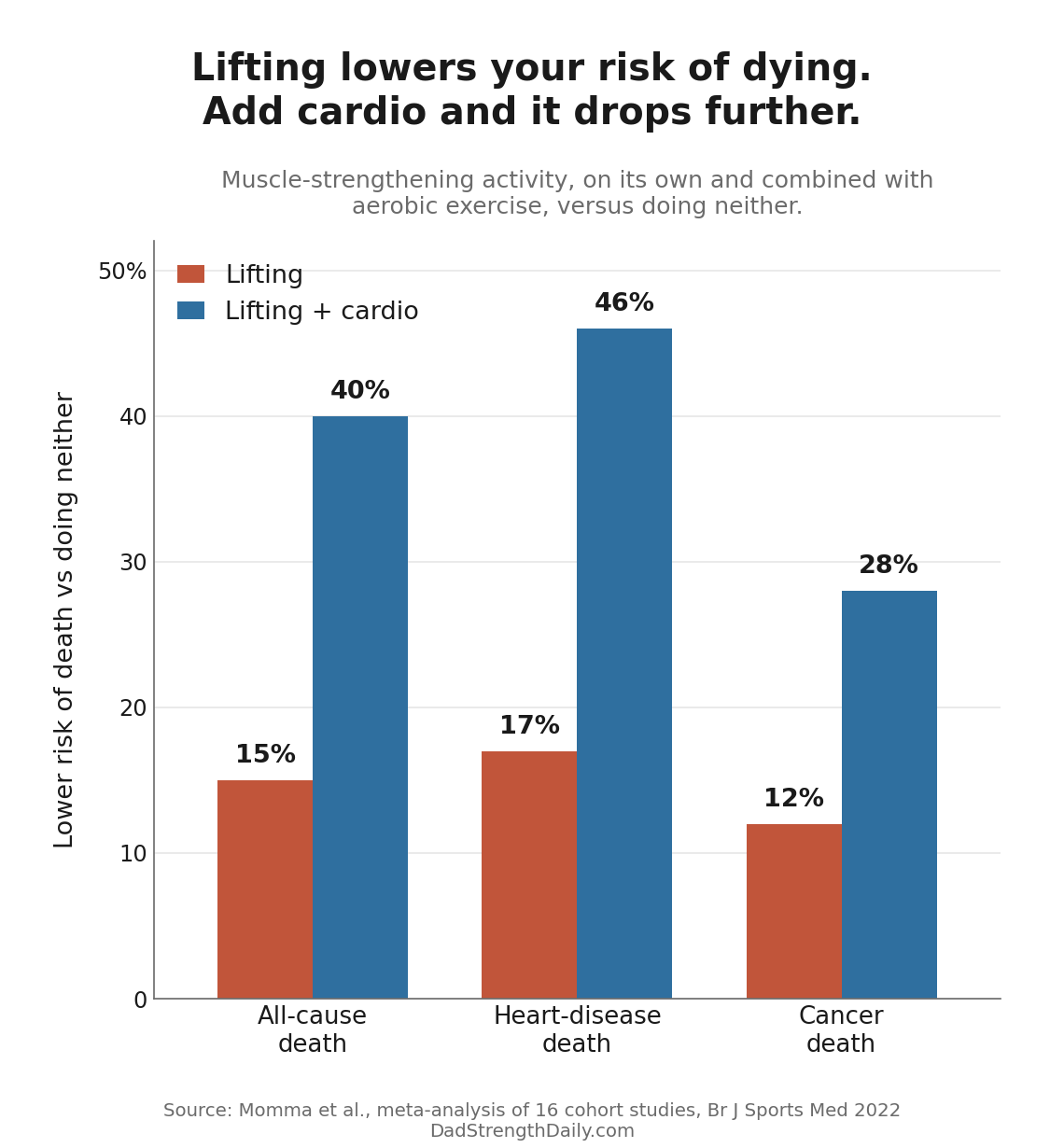
The simplest lever is lifting. Muscle-strengthening activity is tied to a 10 to 17 percent lower risk of dying from any cause, plus lower rates of heart disease, cancer, and diabetes (Momma et al., 2022). And the benefit maxes out at only 30 to 60 minutes a week. Not per day. Per week. Two short sessions capture nearly all of it.
What fades with age isn’t mostly size, it’s strength, and strength is what predicts how the story ends. Grip strength alone is one of the better simple predictors of how long a person lives: in a study across seventeen countries, every 5-kilogram drop came with a 16 percent higher risk of dying (Leong et al., 2015). Left alone, strength drifts down from your forties, until a stumble a stronger body would have shrugged off becomes a broken hip, and for a lot of people that hip is where the real decline starts.
Cardio is the other half, maybe the bigger half. Fitness tracks with survival about as strongly as anything we can measure: in a study of over 120,000 people given an actual treadmill test, the least fit died at dramatically higher rates, and the steepest gains came at the bottom, from simply moving off the couch (Mandsager et al., 2018). You don’t need to be an athlete. I have a bad knee, so I don’t run; I ride a bike indoors and row, and it does the job. I dug into what VO2 max really tells a fifty-year-old in its own piece.
Lifting does quiet work you never see, too: it keeps bone dense, sharpens the balance that keeps you off the floor, and builds cognitive reserve that appears to delay decline, though I won’t pretend it prevents dementia. And it lasts. In a Danish trial, adults near retirement did one year of heavy resistance training and, four years later, still held their leg strength while the non-trainers had measurably declined (Bloch-Ibenfeldt et al., 2024). You can bank strength. It’s never too late to open the account, either: frail nursing-home residents averaging ninety years old did eight weeks of weight training and came out with their leg strength up 174 percent (Fiatarone et al., 1990). If a ninety-year-old can nearly triple hers, fifty is not too late for anything.
What a false alarm gave me
I train five days a week now, in my garage, and it stopped being something I have to talk myself into a long time ago. Most of it is strength work, with a couple of days for conditioning and cardio.

None of it started as fun. It started as fear, and the fear was wrong, but it pointed me at the right door and I walked through. The proof it worked is on a scan I’ve written about: in about six months I added 9 pounds of muscle while losing 44 pounds of fat, in a calorie deficit the whole time, which is not supposed to be the easy case (I broke that down separately). The lifting is why what I lost came off as fat and what I gained went on as muscle. So if you’re losing weight on a GLP-1, lift and eat your protein. Not because the drug is coming for your muscle, but because it’s the cheapest insurance you’ll ever buy.
If you want the non-scary version of how to begin, that’s the how-I-started walkthrough: two or three days a week, the basic movements, a weight that’s honestly hard. Starting is the only genuinely hard part, and it’s a smaller one than the panic makes it look.
Here is what the false alarm actually gave me, and it isn’t the muscle. Most mornings I want to be out in that garage. I like the work, I like watching the numbers crawl up, and I love being fitter than I ever was at 30 or 40. If every study I just cited turned out to be wrong, I’d keep going anyway, because I feel better than I have in my adult life. A fear I no longer believe handed me the best habit I’ve got. I’ll take it.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, and prostate or cancer screening.