
TRT can be real medicine for the right man. But a single low reading on a rushed morning is not a diagnosis, and treating it like one carries a cost a lot of guys never hear about.
I take testosterone, and I’m glad I do. So it catches people off guard when I say I’m wary of how easily a man can end up on it. TRT (testosterone replacement therapy) is real medicine for the right man. But the number-first version of it, a single test followed quickly by a prescription, leaves too much room for a temporary or misleading result to become long-term treatment. It would be easy to hear that as “he’s against testosterone,” and I’m not.
Testosterone has become much easier to test for and get, especially through low-T clinics, telehealth questionnaires, and direct-to-consumer labs. Often a single number is enough to start the conversation about treatment. The trouble is that one testosterone reading tells you almost nothing by itself. A level can come back low for reasons that have nothing to do with needing the drug, and “a low number” and “a man who actually needs testosterone” are not the same thing.
I’m not saying this from the outside. I got there at 52 years old, after real symptoms, low levels confirmed on repeated morning draws, and a workup that pointed at my weight more than my age. The symptoms are what sent me in, and repeated low morning readings confirmed it. None of what follows is medical advice.
Why a low number isn’t a diagnosis
A real diagnosis starts with symptoms, and the symptoms that count are narrower than most men think. The European Male Ageing Study (EMAS) found that a handful of sexual symptoms, low desire, fewer morning erections, and erectile difficulty, were the ones most specifically tied to low testosterone. The physicians at Barbell Medicine make the same point: of the long list of things men blame on low testosterone, only a few really track with it. The fatigue and the brain fog and the flat mood are real, but they’re common to a dozen things, and more often about sleep, stress, or bodyweight than hormones.
Then there’s the number itself, and how you draw the blood matters as much as the result. Testosterone rises and falls through the day, so a real workup uses an early-morning, fasted draw, repeated on a second day. The same reading of 240 means one thing at 7 a.m. after a normal week and something completely different at 3 p.m. on three hours of sleep. And before it counts as a diagnosis, a good clinician rules out what quietly lowers testosterone on its own, excess body fat, poor sleep, heavy drinking, some medications, a recent illness, because addressing those can sometimes bring the number back with no prescription at all.
That’s the standard, and it’s why the Endocrine Society recommends against routinely testing men who have no symptoms. A number pulled off a man who feels fine is a different animal from that careful, symptom-first workup, and the size of that gap is a lot of where my hesitation sits.
What a year of testosterone actually did
The blood draw itself is low-risk. What worries me is what a borderline result can set in motion. Picture a healthy 32-year-old who screens a little low one morning, and the clinic is busy, and nobody repeats the draw or asks why. If he ends up on a prescription, he’s now carrying the downsides of the treatment for a number that was never confirmed.
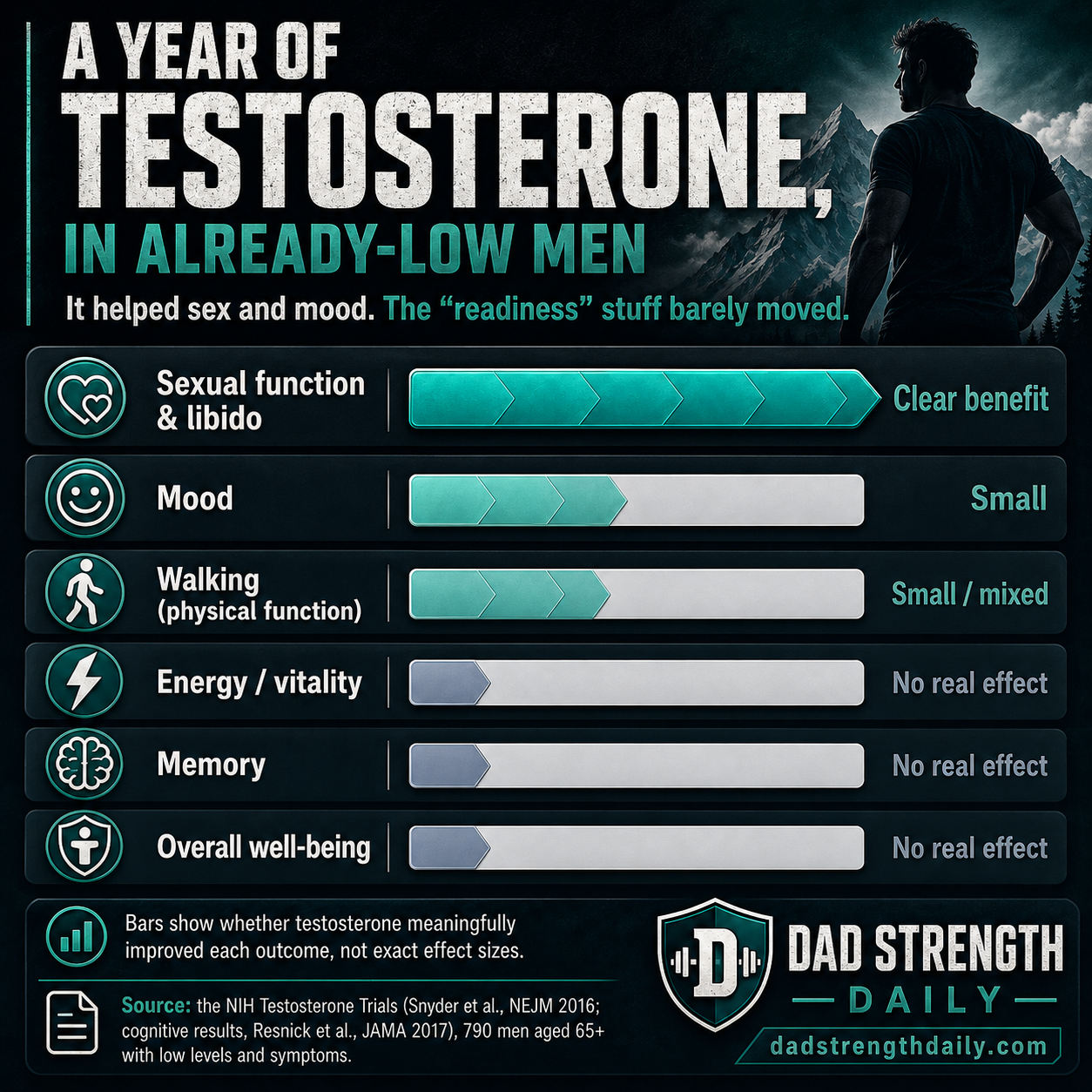
And the case for treating him is thinner than the pitch sounds. I went into the NIH Testosterone Trials expecting a decent argument for it, and didn’t really find one. That study put 790 older men, genuinely low and symptomatic, on testosterone for a year. Their sex lives improved and mood ticked up a little. Energy, walking, memory, the everyday stuff you’d actually hope it fixes, came out small, mixed, or flat, with no real gain in vitality or well-being. And those men were low to begin with. For a young guy whose one-off low reading was never even confirmed, the trial says almost nothing.
Treatment isn’t consequence-free, either. TRAVERSE, the big safety trial, was reassuring on its main question, it didn’t raise major cardiovascular events, but it turned up an unexpected fracture signal: 3.5 percent of the testosterone group had a clinical fracture versus 2.5 percent on placebo. Those men were older and in rougher health than a healthy 32-year-old, so I wouldn’t hang too much on it. Still, it’s a reminder the drug carries its own risks.
The fertility risk I’d want a young guy to know
The fertility hit worries me most, and it’s the part almost nobody brings up. Exogenous testosterone doesn’t simply stack on top of what you already make. It suppresses the signals (LH and FSH) that keep the testicles producing testosterone and sperm, so sperm production can fall sharply and testicular volume can decrease. Fertility guidelines are blunt about it: they advise against testosterone on its own for any man who cares about having kids, now or later.
Most men recover sperm production after they stop, but it can take many months, sometimes up to two years, and it’s less predictable after a long time on the drug, at older ages, or when fertility was already shaky. That’s a lot to take on for a young man who hasn’t started a family, and especially for a number that might have been fine. If there is one thing I’d want a young guy to hear before he says yes, it’s this one. And fertility may not be the deciding issue for every man over 50, but the larger point holds: starting testosterone suppresses your own production and turns a borderline lab result into an ongoing treatment decision.
Who this could actually help
None of this means testosterone is a scam. Real hypogonadism is common and badly undertreated, and plenty of men who genuinely have it suffer for years before anyone takes it seriously. Those men should be easier to treat, not harder. My problem isn’t treatment. It’s the sorting: symptoms are where the evaluation should start, and testing without that context can flag men who don’t have clinical hypogonadism.
Where I land
Testosterone is getting easier to get, too. Recently, the FDA requested that drugmakers remove the label language saying TRT’s safety and effectiveness hadn’t been established for age-related low testosterone. That points in a more permissive direction, though it isn’t the same as approving testosterone for ordinary aging.
So, as a guy who takes the stuff and is glad he does: don’t let one number make the call. If the symptoms are there, get it confirmed on a second morning draw, rule out the boring explanations first, the weight, the sleep, the drinking, and know what you’re signing up for before you start. I’ve written up my own TRT, and I’ll defend it all day for the man who needs it. TRT can be life-changing. So can a rushed diagnosis, just not the way he was hoping.
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.