
A new ingredient just cleared the FDA, the first in twenty years. It sent me looking at what sunscreen actually does, where the fear is overblown, and whether a fair-skinned guy in Boston needs to think about it more than a couple of times in the summer.
I am about as fair as a person gets. My family is from Hamburg, up where northern Germany starts to blur into Scandinavia, and I have the skin to prove it. I burn on overcast days. I am the exact person sunscreen was invented for, and for most of my fifty-three years I have treated it as a thing you grab once a year before a beach trip.
Turns out I have company. In the most recent national survey, only about 12 percent of American men said they always use sunscreen when they are out in the sun for more than an hour. For women the figure was 29 percent (CDC, National Health Interview Survey, 2020).
What finally got me to read the science was a piece of news that sounds pretty dull. This month the FDA approved bemotrizinol, the first genuinely new sunscreen ingredient cleared in the United States in more than twenty years. If you keep hearing that the famous Korean and European sunscreens are finally coming to America, this rule change is why, though that door is open only a crack. So I went looking.
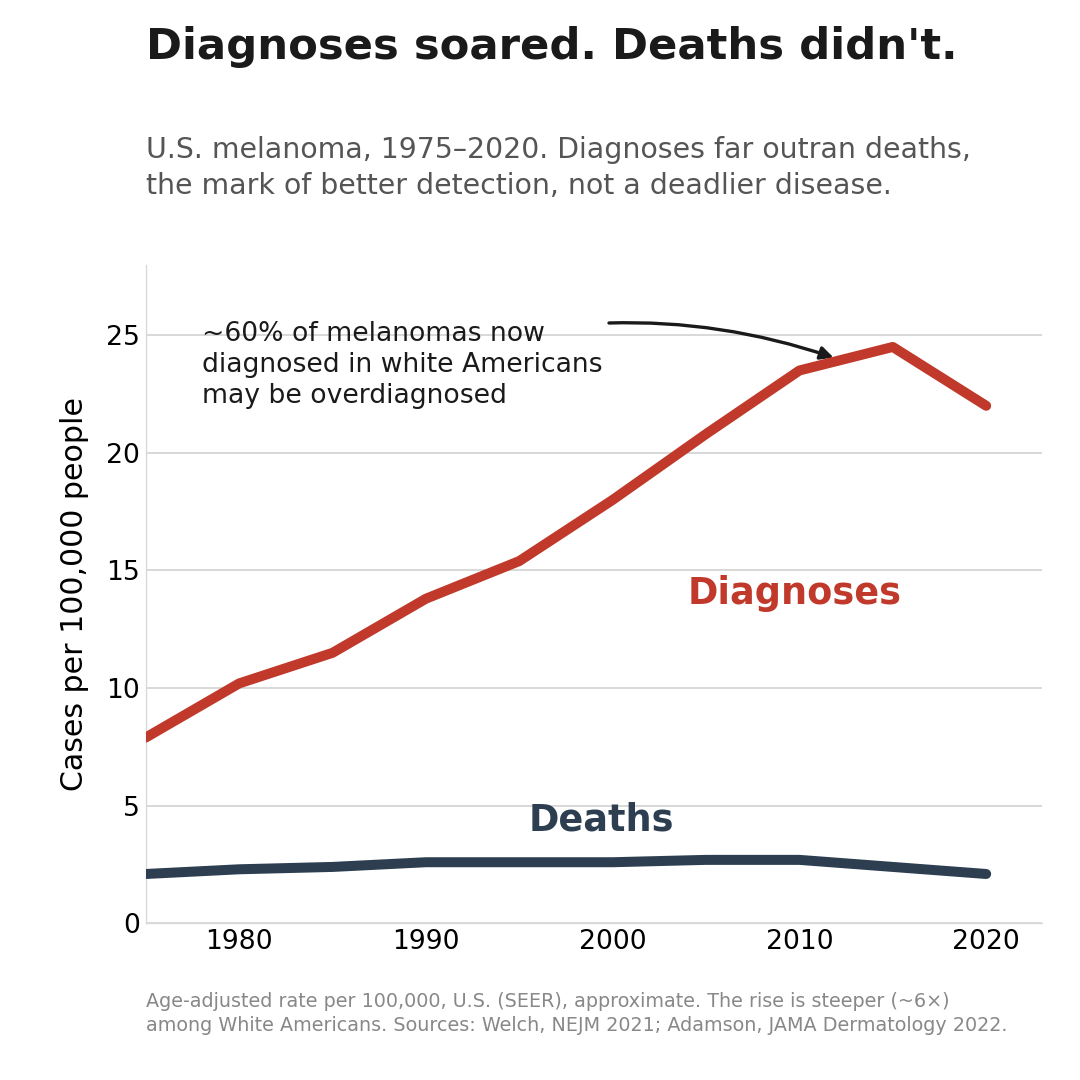
The melanoma “epidemic” is partly an epidemic of looking harder
The first number I ran into stopped me. Since the 1970s, the rate at which Americans get diagnosed with melanoma has risen roughly sixfold. Over the same stretch, the death rate rose only a fraction as fast (Welch, Mazer, and Adamson, New England Journal of Medicine 2021). When a cancer is truly becoming more common, deaths usually climb with it, unless better treatment or earlier detection is holding them down. Here they did not climb much at all. I had assumed the scarier version was just true.
Most epidemiologists chalk it up to overdiagnosis. As awareness campaigns and aggressive screening sent more people in for more biopsies, pathologists began catching a flood of tiny early lesions that meet the technical definition of melanoma but would never have harmed anyone. No one can tell at the moment of the biopsy which of those tiny lesions is harmless and which is the rare killer, so they all get treated. One analysis estimated that around 60 percent of melanomas now diagnosed in white Americans fall into that harmless-but-labeled bucket (Adamson et al., JAMA Dermatology 2022).
This is tricky news, because it cuts both ways. Melanoma is real and it still kills more than 8,000 Americans a year, and finding a truly dangerous one early saves lives. But the story that we are living through a runaway, sun-driven cancer wave is mostly a story about how hard we have started looking, not how much more dangerous the sun became. Sun protection earns its place on its own merits. You do not have to be frightened into it.
What sunscreen is actually proven to do
So if the melanoma panic is overcooked, does sunscreen earn its keep at all? Here the evidence is narrower and stronger than the marketing. Most of it traces back to one unusually rigorous trial in Nambour, Australia, where researchers randomly assigned about 1,600 adults to either daily sunscreen or use-it-when-you-feel-like-it, then followed them for years. The daily group developed significantly fewer squamous cell carcinomas, one of the two common skin cancers (Green et al., Lancet 1999). A decade after the trial ended, they also had fewer melanomas, and the drop in invasive melanoma, the kind that actually kills people, was large enough to count statistically (Green et al., Journal of Clinical Oncology 2011). A separate look at the same group found their skin aged measurably less: 24 percent less photoaging over four and a half years (Hughes et al., Annals of Internal Medicine 2013).
That part is hard to argue with. Daily sunscreen cut squamous cell carcinoma and slowed wrinkling, with a real signal on invasive melanoma on top. If you care about any of that, it does the job.
The number on the bottle mostly measures how much you skip
When I was a kid, SPF 15 was standard and SPF 30 sounded paranoid. Now the shelf starts at 50 and runs to 100. Some of that is plain number inflation, because a bigger figure sells. The math behind it is less impressive than it looks. SPF 30 blocks about 97 percent of the burning UVB rays. SPF 50 blocks about 98. Going from 30 to 50 buys you a single percentage point.
The catch is what happens outside the lab. Those ratings come from technicians applying a thick, precise dose almost nobody matches in real life. Studies keep finding that people use a quarter to half of the tested amount, and protection falls off fast when you go thin. Applied the way a normal person applies it, an SPF 50 performs more like an SPF 14. So the high number is less a promise than a cushion for the fact that you will under-apply. The brand matters less than whether you put on enough, roughly a shot glass for the body and two fingers’ worth for the face and neck, and whether you put it back on.
The number hides one more thing. SPF only rates UVB, the rays that burn. It says nothing about UVA, which penetrates deeper into the skin, drives aging, and slips through the car and office glass that blocks most UVB. There is a well-known medical photo of a truck driver whose left side, the window side, aged decades faster than his right after twenty-eight years on the road (New England Journal of Medicine, 2012). For UVA protection you have to look for the words “broad spectrum,” not a big SPF.
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
Mineral, chemical, and the bloodstream scare
The other thing that spooked people away from sunscreen was a pair of FDA studies showing that the chemical filters in most products get absorbed into the bloodstream, several of them well above the agency’s testing cutoff (Matta et al., JAMA 2019 and 2020). Oxybenzone, the most controversial filter, showed up in blood at striking levels. The headlines ran with it.
I think the headlines ran past what the studies showed. They found absorption. They did not find harm. And that cutoff is not a danger line. It is just the level above which the FDA wants a company to run the safety tests the industry had skipped for decades, on the assumption these molecules stayed on the surface. The agency said plainly this was not a reason to stop using sunscreen. No solid human evidence says those blood levels cause harm. No proof says they are perfectly fine either, which is a fair reason to hedge if you want to.
If you do want to hedge, the mineral filters, zinc oxide and titanium dioxide, are the move, and one myth is worth killing here. Mineral sunscreens do not work by sitting on your skin like tiny mirrors. They mostly absorb UV and convert it to heat, the same as the chemicals do, and reflect only a few percent. They are not magic. They are the two filters the FDA rates as generally recognized as safe and effective, and they barely absorb. The tradeoff is the white cast that makes them a harder sell, which is exactly the problem the new ingredient was built to fix. I reach for a mineral one when I reach for anything, mostly because it seems a safe, easy choice and I will actually keep it around.
Why one new ingredient is a real story
On June 9 the FDA cleared bemotrizinol, the first new sunscreen active ingredient approved in this country since the late 1990s (FDA, 2026). Europe and parts of Asia have had it for twenty years, because they regulate sunscreens through different systems that have moved newer UV filters to market faster than our over-the-counter drug process. Congress tried to force the issue in 2014 and got nowhere. A 2020 law finally rebuilt the process, and bemotrizinol is the first thing through the door. Manufacturers can start putting it in products on August 9, though new formulas take time to develop and ship, so do not expect it at the drugstore overnight.
It is also one filter, not the floodgates. The sunscreens people rave about from Seoul and Paris lean on a whole palette of modern UV filters, most of which the FDA still has not cleared. Bemotrizinol is the first crack in a door that has been stuck for a generation.
I care about it for a simple reason: it goes after the two problems I just walked through, at the same time. It is genuinely broad spectrum, with the kind of UVA coverage the US market has lacked. It stays stable in sunlight, unlike older UVA filters that break down while you wear them. And it is a big enough molecule that it barely absorbs, which largely sidesteps the bloodstream question. Formulated well, it manages all of that without the white cast, so it is pleasant enough that people might actually wear it. Two honest caveats. The “American sunscreen is hopelessly behind the world” line you hear from influencers is overstated, because a good high-zinc mineral product already protects you fine. And no one has run the decades-long trial proving that people who use bemotrizinol get less skin cancer; what it has is twenty years of use in Europe and a clean safety and absorption record. But more options people enjoy using is the whole ballgame, because the best sunscreen is the one you will put back on.
The skin cancer sunscreen won’t solve
I did not know this part, and I am glad I read it. There is a stubborn myth that people with dark skin do not get skin cancer. They get it far less often, which is true, but when they do, they are more likely to die of it. In a study of more than 200,000 men, five-year melanoma survival was 75 percent for white men and about 52 percent for Black men (Fernandez et al., Journal of the American Academy of Dermatology 2023). As the father of two Black sons, that gap got my full attention.
Some of it is late diagnosis driven by the myth itself. Some of it is biology. The melanoma that most often appears in darker skin, acral lentiginous melanoma, shows up on the palms, the soles of the feet, and under the nails, places the sun barely touches. It is the cancer that killed Bob Marley, who reportedly waved off a dark spot under his toenail as a soccer injury. Sunscreen is not the main tool against this kind, which means “wear sunscreen” misses the point here. The useful advice is to check the soles, the palms, and the nail beds, and to take a new dark streak under a nail, a changing spot on a sole, or a sore that will not heal seriously no matter your skin tone. That one is going up on the wall in my house.
What a fair-skinned guy in Boston is actually going to do
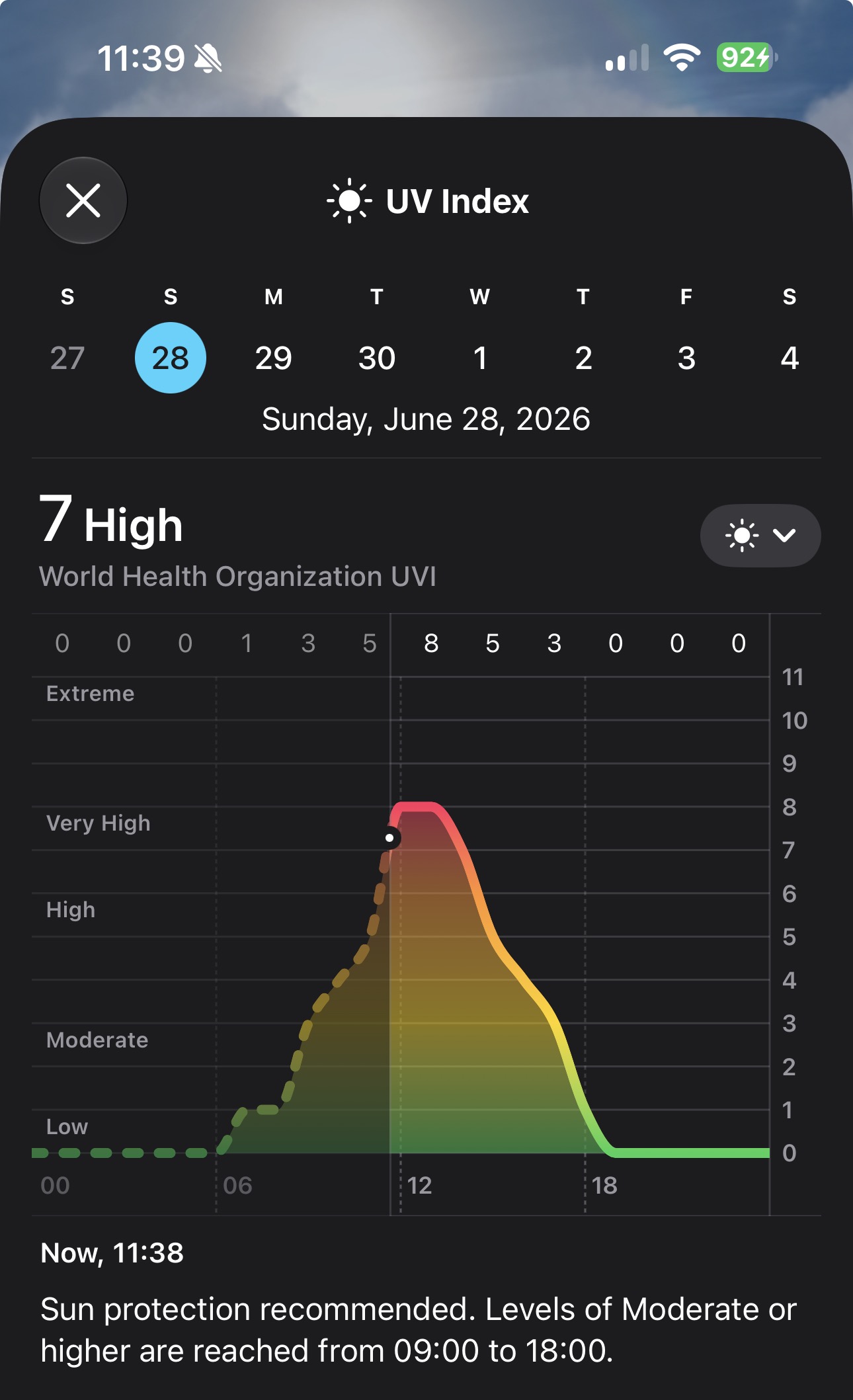
I am not about to become a man who slathers up 365 days a year, and the evidence does not ask every Bostonian to treat a January sidewalk like a July beach. The smarter rule is to watch the UV index, the little number buried in your phone’s weather app, instead of the calendar. I checked mine this past Sunday, a sunny late-June afternoon in Boston, and it read 7, which the app calls high, with sun protection flagged from nine in the morning until six at night.
When it reads 3 or higher and I will be outside for a while, I will put some on. In Boston that mostly means late spring through early fall, plus the obvious ones: the beach, and skiing, where the snow bounces UV back up into your face and the altitude makes it stronger.
In a Boston winter the index sits at 1 or 2, and for most people the cancer benefit of everyday sidewalk sunscreen then is small, snow glare and photosensitizing medications aside. At our latitude your skin also makes almost no vitamin D from the winter sun, something that was measured on Boston rooftops years ago, so covering up costs you nothing there either. Get your vitamin D from a capsule in January, not by burning in July.
Most sunscreen advice is written as if everyone lives in Arizona. If you do live in the Sun Belt, it is closer to right, because Florida, Texas, and the desert Southwest run a high UV index for much of the year. The rest of us get to be seasonal. Either way the honest rule is the same, and it is neither the calendar nor the map: it is the UV index. Mine is boring. I check the index instead of the season, I use more than I used to, and I’ll consider wearing a hat, which fixes half the problem and never washes off. And as a fair guy from the top of Germany who is squarely in the lazy 12 percent, this is the summer I stop treating the one thing my skin obviously needs as optional.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.