
I take tirzepatide. So when the headline came through this week that GLP-1 drugs might slow the spread of cancer, it intrigued me more than most drug news. This is the medication in my own refrigerator. I went and read the actual study instead of the headline, and the short version is that the signal is real and genuinely interesting, and it is also nowhere near a reason to take one of these drugs for cancer.
Here is what was presented.
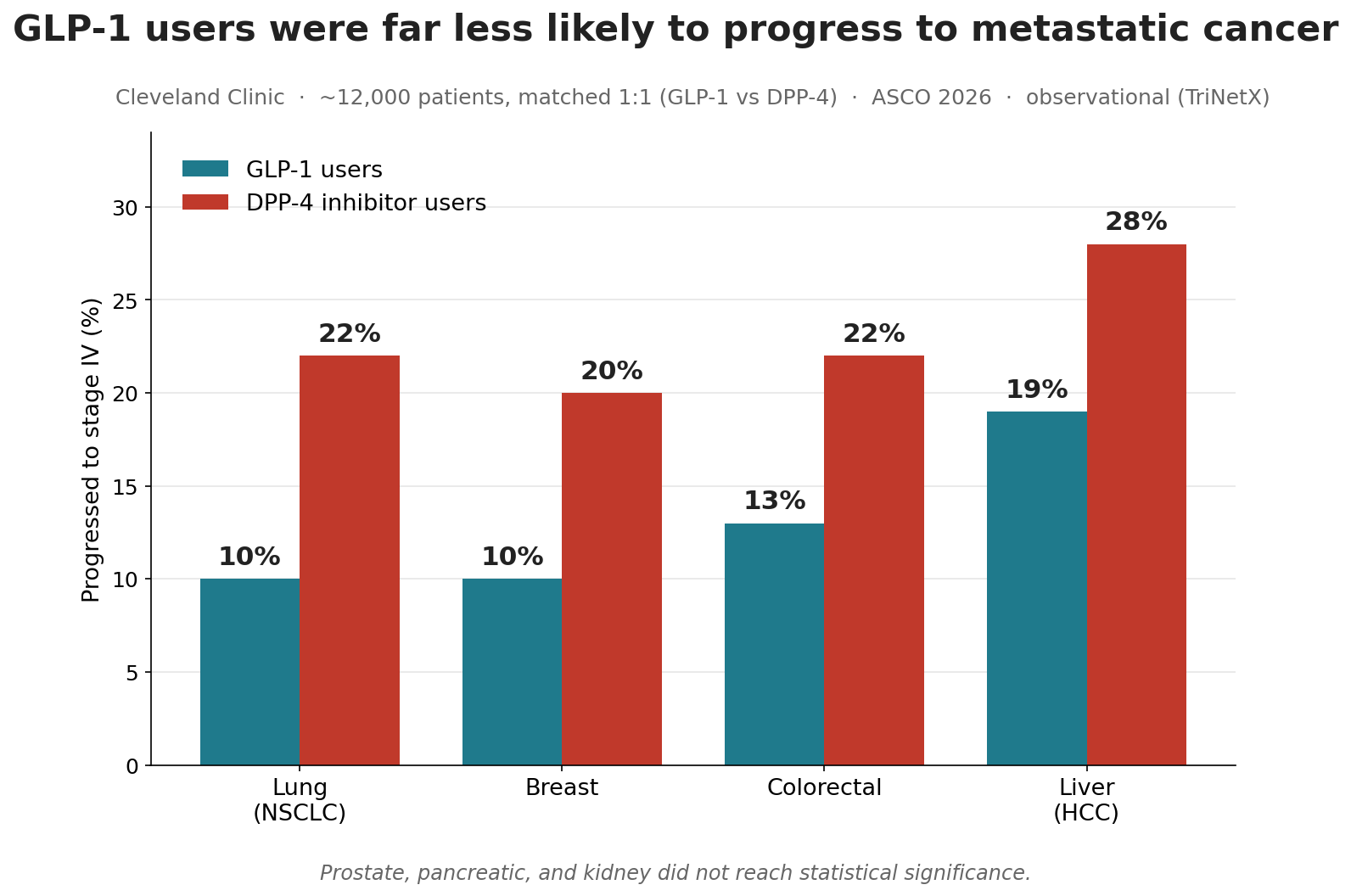
What the Cleveland Clinic data showed
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
The study came out of the Cleveland Clinic and was presented at the big American Society of Clinical Oncology meeting in Chicago as Abstract 3143. It used TriNetX, a research network pulling deidentified records from more than 150 million patients. The team found 10,225 people who started a GLP-1 drug after being diagnosed with an early-stage cancer, stage I to III, and matched each one head to head with a comparable patient who started a different diabetes drug, a DPP-4 inhibitor, about twelve thousand patients in all. They balanced the two groups on age, race, body weight, other illnesses, and cancer treatment, then watched to see who progressed to stage IV.
For four of the seven cancers they looked at, the people on GLP-1 drugs were far less likely to progress. In non-small-cell lung cancer, progression dropped from 22 percent to 10. In breast cancer, from 20 to 10. In liver cancer, from 28 to 19. In colorectal cancer, from 22 to 13. Those are large gaps, hazard ratios in the range of 0.5 to 0.7, and all four cleared statistical significance.
Prostate and pancreatic trended in the same direction, but not by enough to rule out chance, and kidney showed no significant benefit at all. That selectivity actually makes the result more believable, not less. A drug that improved every cancer equally would look like a measurement artifact. A drug that helps some and not others looks more like biology.
Why this is better than the usual GLP-1 headline
Most of the “Ozempic also cures X” stories compare people on the drug to people on nothing, which is a trap, because the people who get prescribed and can afford these drugs tend to be healthier and better cared for to begin with. This study did something smarter. It compared GLP-1 users to people on another diabetes drug. Both groups had diabetes, both were motivated enough to be on treatment, both were in the medical system. That does not erase the bias, but it cuts into it. The researchers also dropped anyone who progressed within the first three months, which keeps the sickest patients from skewing the picture at the start.
There was a second piece I found more persuasive than the headline numbers. The team looked at tumor tissue and found that cancers expressing more GLP-1 receptor had lower death rates, about a third lower overall and close to half in breast cancer. That is the kind of mechanistic thread that makes an association look less like an accident. The drug binds a receptor, and the tumors carrying more of that receptor did better.
And there is a reassurance buried in here for anyone already taking one of these. For years the open question ran the other way, whether GLP-1 drugs might raise cancer risk. The senior author put it plainly, that it is reassuring they found no signal suggesting these drugs cause a wave of cancer over the next decade. If you are on tirzepatide or semaglutide and that worry has nagged at you, this is the opposite of bad news.
The catch, and it is a real one
Now the brakes. This is an observational study built from insurance and health-record data, and the lead author said so himself, that the associations are strong but there are covariates the database may not capture. Observational data can tell you two things move together. It cannot tell you one caused the other.
When you go looking for the randomized evidence, the kind that actually establishes cause, it thins out fast. A network meta-analysis published last year pooled 67 randomized trials and more than 200,000 patients, and the only GLP-1 drug that reached significance for fewer metastatic events was a minor one called efpeglenatide. Even that came from cancers reported incidentally in trials designed to study diabetes, not cancer. Nobody has run a trial built to test whether a GLP-1 slows cancer spread. The oncologist ASCO put forward to comment on the study said the same thing, that the consistency across tumor types is what is new, and that data this large warrants a proper randomized trial.
So we have a big, internally consistent observational signal, a plausible mechanism, and almost no randomized proof. That is a real finding at an early stage. It is not a treatment.
What I am doing about it
Nothing, and I would tell you to do nothing too. I take tirzepatide because of where my weight and metabolic numbers were, and any cancer benefit, if it turns out to be real, is a bonus I did not plan for. I am not going to start treating it as cancer insurance, and it is the same reason I am skeptical of microdosing these drugs for unproven perks. Nobody should start a GLP-1, or stay on a gray-market version of one, on the strength of a conference abstract.
If you already take one of these for the reasons they are actually approved for, this is a quietly encouraging piece of a much larger puzzle. If you do not, it is a reason to watch the trials, not to call your doctor. The interesting part here is the receptor, not the headline, and the next real answer comes from a trial nobody has run yet.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.