
The seven levers ranked by what the evidence says they’re worth, with the studies linked and the junk cut.

Rewritten from the ground up in June 2026. The old version of this page oversold a few studies and carried affiliate links. Both are gone, and every number below links to the actual paper.
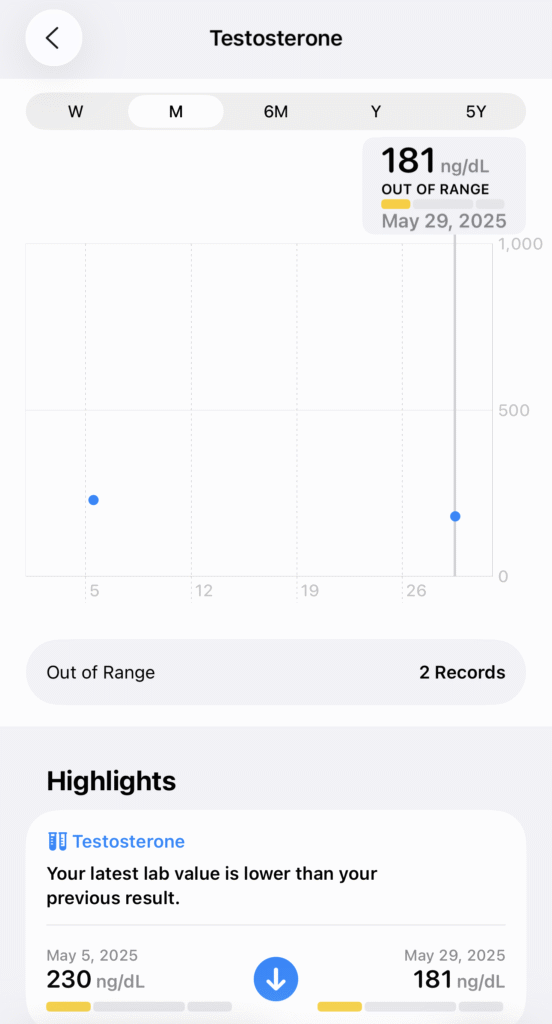
I tested my total testosterone twice in my early fifties. The first draw came back at 230 ng/dL. The retest, which I had half hoped would clear things up, came back at 181. The American Urological Association treats anything under 300 ng/dL as supporting a diagnosis of low testosterone, and I was under it twice, with the energy and motivation to match.
So this is not a theoretical topic for me. I spent a long time working the natural levers before I ever talked to a doctor about anything stronger, and I would work them in the same order again. (My starting point was the annual physical where reality caught up with me.) That order is the point of this post. The seven things below are not equal. One of them can move your number by triple digits. Two or three are worth maybe ten to fifteen percent. One barely moves the number at all and earns its place anyway. The rest are rounding errors with good marketing budgets.
Body fat is the only triple-digit lever
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
1. Lose the extra weight
Testosterone does decline with age. The Baltimore Longitudinal Study of Aging pegged the drop at roughly one percent a year and found outright low-testosterone values in about one in five men over 60. But age is the lever you cannot pull. Weight is the one you can, and it is far more powerful than most men assume.
A meta-analysis of 24 studies of obese men who lost weight found that diet-driven weight loss raised total testosterone by an average of about 83 ng/dL. Men who lost much more weight through bariatric surgery gained an average of 252 ng/dL. 252, from losing weight. No supplement on the market does a tenth of that. The same analysis found that the single best predictor of how much your testosterone rises is simply how much weight you lose.
The mechanism is not mysterious. Fat tissue runs an enzyme called aromatase that converts testosterone into estradiol, so the more fat you carry, the more of your testosterone gets siphoned off. The insulin resistance that comes with belly fat also quiets the signal your brain sends to your testes in the first place. Lose the fat and both problems shrink with it. A European study that followed 2,395 middle-aged and older men for four years watched it happen in both directions: men who gained weight drifted down, men who lost weight climbed back.
I lost about 170 pounds after fifty. Testosterone wasn’t why I did it, and it sure wasn’t fast. But if your total T is in the 200s and you are carrying 40 extra pounds, the scale is where the real money is. Everything else on this list is fighting over scraps by comparison. One honest caveat: the response varies man to man, and if the problem sits in the testes themselves rather than the signal reaching them, weight loss alone may never get you to normal. That distinction matters at the end of this post.
Five hours of sleep cost those men 10 to 15 percent
2. Protect seven hours
The cleanest causal evidence on sleep and testosterone is a small JAMA experiment that took ten healthy young men and capped them at five hours in bed for eight nights. Daytime testosterone fell 10 to 15 percent, which in their case meant dropping from around 530 to 476 ng/dL in a single week.
I want to be straight about the limits of that study: ten guys, all in their twenties, one week. Nobody has run the same protocol on 55-year-olds. But one bad week of sleep costing you the equivalent of a decade of natural decline is the kind of result I take seriously, especially because sleep is also the foundation the other levers either stand on or don’t.
Also: if you snore, wake up unrefreshed, or your wife has watched you stop breathing at night, get a sleep study before you spend a dollar on anything else in this post. Sleep apnea is common in heavy middle-aged men and it shreds exactly the deep sleep your hormone production depends on. Treating apnea will not turn you into a 25-year-old, but ignoring it quietly caps everything else you try. I wrote up my own sleep experiments, including the parts that didn’t work, separately.
3. Keep lifting, but not for the testosterone
The old version of this post claimed that compound lifts could raise testosterone 15 to 20 percent in eight weeks. I went looking for the study behind that claim and could not find it, because as far as I can tell it does not exist. What the exercise literature consistently shows instead: heavy squats and deadlifts produce a testosterone spike, but it is transient, gone within about an hour, and study after study has failed to show training programs meaningfully raising the resting level you would see on a morning blood draw.
So why does lifting stay on the list? Because almost everything low testosterone takes from you, training gives back directly. Strength, energy, body composition, mood. All of it responds to a barbell whether or not the blood number moves. Muscle also improves insulin sensitivity, which feeds the weight-loss lever above. And if you ever do end up on hormone therapy, every benefit of it lands better with training underneath.
I lift in my garage and I would keep doing it even if it lowered my testosterone. It pays out in too many other ways.
Dietary fat matters a little, alcohol can matter more
4. Don’t cut fat below a quarter of your calories
There is a real finding here, just a smaller one than the internet wants it to be. A meta-analysis of six controlled feeding studies, 206 men in total, found that moving men onto low-fat diets lowered total and free testosterone by a modest but consistent amount. The likely reason is boring biochemistry: dietary fat and cholesterol are upstream raw material for steroid hormones. To be clear about what that is not saying: this is a modest diet-pattern effect in controlled studies, not a cholesterol-in, testosterone-out equation you can eat your way up.
Don’t try to lose your weight on an extreme low-fat diet. Keep fat somewhere around 30 percent of calories, get it from food you would eat anyway (eggs, olive oil, fish, nuts, the occasional ribeye), and spend your discipline budget on the calorie deficit instead. What this finding is not: a license to go full carnivore. If a high-fat diet makes you gain weight, you have traded a small lever for the big one, in the wrong direction.
Carb timing around workouts, which used to have its own section on this page, has no credible testosterone evidence behind it at all. That kind of false precision is exactly what keeps men busy while the real levers sit unpulled.
5. Look honestly at the alcohol
I drank plenty in my twenties, in 1980s Germany, where it more or less came with the territory, and I quit completely in my forties, mostly because it gave me headaches and had stopped giving me anything back. No preaching here. Two beers on a Saturday will not show up in your labs.
Several drinks a night is a different story. In heavy drinkers, alcohol suppresses testosterone production directly, and well before that threshold it ruins the deep sleep production depends on. If that describes your week and you wonder why your energy is gone at 52, the honest experiment is a dry month and a blood test, not a supplement order.
Supplements correct deficiencies, they don’t add bonuses
6. Test before you supplement
Vitamin D is the honest poster child for this whole category. In a one-year randomized trial of 54 overweight men who were all vitamin D deficient, about 3,300 IU a day raised total testosterone by almost 80 ng/dL while the placebo group went nowhere. Encouraging. But when a 2024 meta-analysis pooled all 17 randomized trials, deficient and non-deficient men together, the average gain was 11 ng/dL and free testosterone did not move at all.
I read those two results this way: if you are low, fixing the deficiency can genuinely help. If you are not, you are buying hope. A blood test settles which one you are, it costs less than two months of supplements, and any generic D3 works if you do need it. Zinc runs on the same logic. A true zinc deficiency suppresses testosterone, and zinc on top of a normal level is expensive urine.
Test first, supplement second. The booster aisle sells it in the other order for a reason. The aisle is one corner of a bigger pattern: at some point, biohacking just becomes shopping.
7. Ashwagandha, the last booster standing
Out of the entire testosterone-booster aisle, only one ingredient I have found has a placebo-controlled trial in middle-aged men worth talking about. A 2019 crossover study gave overweight men aged 40 to 70 an ashwagandha extract for eight weeks and measured total testosterone 14.7 percent higher than placebo. The previous version of this post said 17 percent. That was wrong; the higher figure belonged to DHEA-S, a different hormone in the same study.
What the supplement companies never quote is that the men did not feel any better. Fatigue and vigor improved just as much on placebo. The hormone moved on the lab report and nowhere else. My own n of 1 matched the placebo arm, except with headaches, so I dropped it. And natural does not mean automatically harmless: extracts and doses vary wildly by brand, there are case reports of liver injury, and if you take thyroid or sedative medication this is a conversation with your doctor, not an impulse buy.
As for the rest of the aisle: creatine is a fine training supplement, but take it for your muscles, not your hormones, because the claim that it raises DHT rests on a single small study of rugby players. How much of it to take is its own argument, and I worked through the case for and against pushing the creatine dose higher separately. Tribulus, D-aspartic acid, boron blends, anything with a chrome wolf on the label. No. If a $40 bottle could add even 50 ng/dL in men like us, the meta-analyses would have found it by now.
Two labs under 300, and what I did next
This is where I am supposed to tell you the seven levers fixed me. They didn’t, not all the way.
Both of my tests came back under the AUA’s 300 ng/dL line, with symptoms to match, and my two draws came in 49 ng/dL apart, which tells you something useful all by itself: this hormone bounces around. Test in the morning, when levels peak, and test twice before you conclude anything. Ask for the full panel rather than the single number: total T, free T, SHBG (the protein that binds testosterone and decides how much of it your body can actually use), and estradiol. Then have a doctor interpret it instead of a forum. It is also worth ruling out the quiet suppressors while you are at it: untreated sleep apnea, opioid painkillers, and long-term steroid medications like prednisone all push the number down.
If after six months of honest work on the real levers, weight and sleep above all, you are still under 300 with symptoms, then TRT is a legitimate medical decision, not an admission that you failed at push-ups. I eventually made that decision myself, through Marek Health (I am a customer, not an affiliate, and they don’t know I’m writing this). If you go down that road, I would want an actual doctor watching it closely. Labs every three to six months, not a mailed vial and a wink. Conservative dosing, split into smaller injections across the week instead of one big weekly shot. Someone who tracks your hematocrit (red blood cell concentration, which TRT pushes up) and your estradiol. And someone who asks whether fertility still matters to you before the first prescription, because TRT suppresses sperm production while you are on it.
And none of it retires the list above. Hormone replacement on top of bad sleep and 40 extra pounds is paying a monthly fee to fight your own habits.
I still work every lever on this page, and they work better than they did when I weighed 170 pounds more. What changed is that I stopped expecting them to do a job my labs had twice told me they couldn’t.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.