
I keep getting asked some version of this question. People on tirzepatide want to know if brenipatide is the upgrade. People reading about brenipatide want to know how it stacks up against the drug everyone is already on. The honest answer is that the two drugs are in the same broad family but they are being developed for very different problems, on very different timelines. They will be available for different primary indications, i.e. your doctor will likely be able to prescribe Brenipatide for alcohol abuse even if you are not overweight and insurance will hopefully cover it.
Quick version: tirzepatide is the obesity and type 2 diabetes drug already in millions of fridges. Brenipatide is Lilly’s monthly-dose follow-up molecule that is being studied first for alcohol use disorder, not for weight loss. They share a drug class. They do not share an indication. If you are trying to lose weight in 2026, tirzepatide is the answer. If you are following the science on what comes next, brenipatide is the more interesting story.
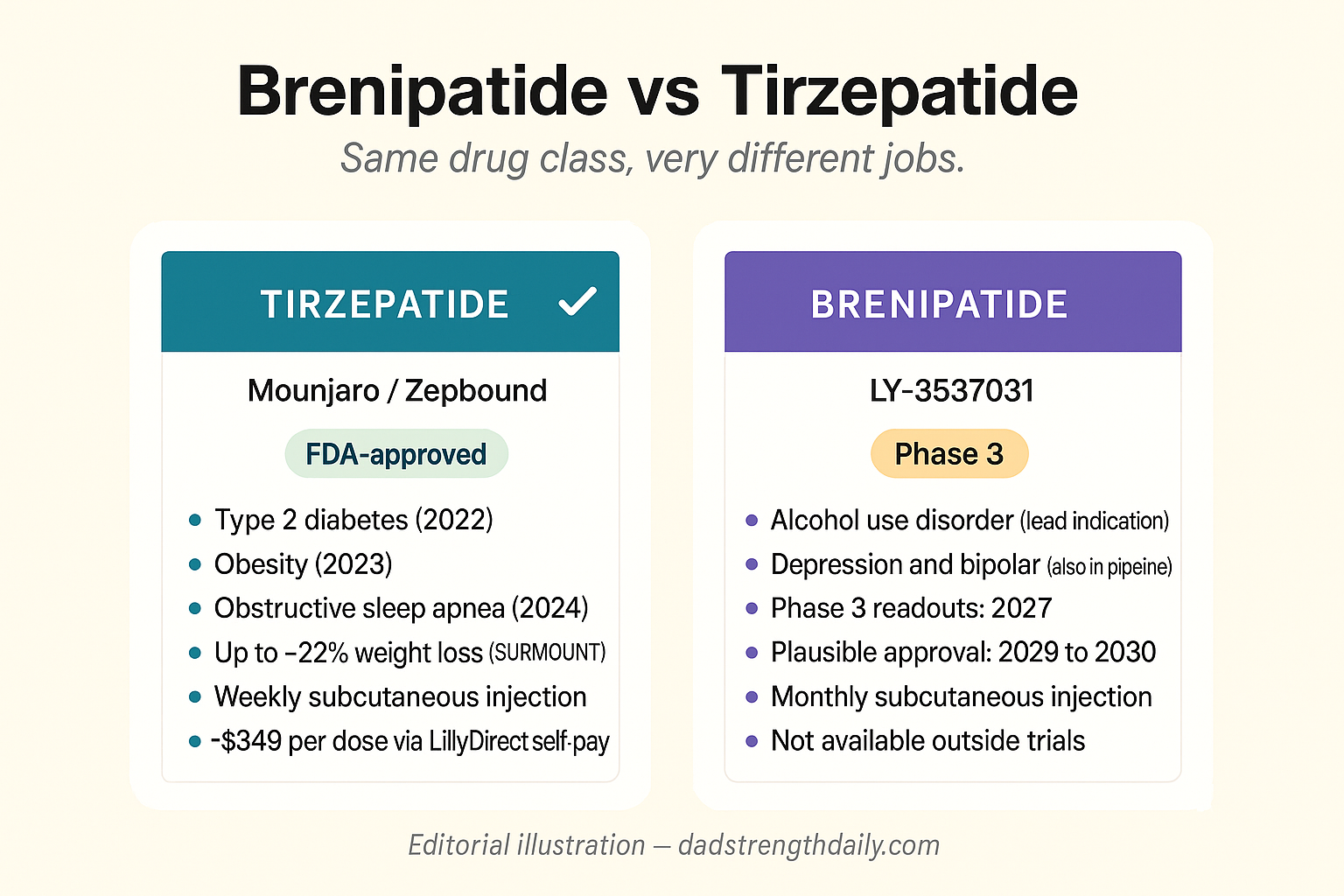
Two drugs from the same company, very different jobs
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
Both drugs come out of Eli Lilly, and both are dual agonists of the GLP-1 and GIP receptors. That is where the surface similarity ends. Lilly’s own pipeline groups them differently. Tirzepatide sits in the Cardiometabolic Health bucket. Brenipatide is in Neuroscience. The drugs were engineered for different jobs and Lilly is testing them in different patient populations.
Tirzepatide is the active ingredient in Mounjaro and Zepbound. It has been FDA-approved since 2022 for type 2 diabetes and 2023 for obesity, and Lilly has now added obstructive sleep apnea to the label. It is sold in weekly subcutaneous injections at five doses from 2.5 mg through 15 mg, and the Phase 3 SURMOUNT trials showed average weight loss of roughly 20 to 22 percent at the highest dose over 72 weeks. Tirzepatide is what most people now mean when they say “the weight loss drugs.”
Brenipatide is, in industry shorthand, LY-3537031. It is currently in Phase 3 for alcohol use disorder (the RENEW-ALC-1 and RENEW-ALC-2 trials, 1,100 patients each) and in earlier-stage development for bipolar disorder, major depressive disorder, smoking withdrawal, asthma, cardiovascular and liver disorders, and obesity. Trial readouts on the AUD program start landing in 2027. If those are positive, Lilly is plausibly looking at a 2028 FDA submission and a 2029 or 2030 launch.
That timing matters and I will come back to it.
What tirzepatide already delivers
Tirzepatide has done the thing all drug candidates are eventually judged on. It got through Phase 3 and into commercial use, at scale, and the real-world data keeps lining up with the trial data.
The headline number is the SURMOUNT-1 weight loss result. Average loss at the highest dose was about 22.5 percent of body weight over 72 weeks in adults with obesity and no diabetes. That number lands somewhere between gastric sleeve and gastric bypass in efficacy. Diabetic patients on Mounjaro see roughly 12 to 15 percent body weight loss along with strong glycemic control. The drug is now also approved for obstructive sleep apnea in adults with obesity, where it cut the apnea-hypopnea index by about half in the SURMOUNT-OSA trial. I have been on Zepbound myself long enough to confirm that the trial numbers map to the real-world experience. I also wrote up the SURMOUNT-MAINTAIN dose-reduction trial separately, which addresses what most people want to know once they have hit their target weight.
On availability, tirzepatide is what is actually in pharmacies. Lilly sells it as Zepbound through retail pharmacies and through LillyDirect starting at $299 per month of the lower strengths, which is a substantial discount from the list price for self-pay patients. Insurance coverage varies, and Medicare does not currently cover Zepbound for obesity, though the Medicare GLP-1 bridge demonstration starting July 2026 is a separate path worth knowing about if you are aging into Part D.
On the side effect profile, tirzepatide is well characterized at this point. Nausea, vomiting, constipation, and the general gastrointestinal package are real and dose-dependent. About 6 to 7 percent of patients discontinue for side effects in the pivotal trials, which is the benchmark every next-generation GLP-1 is now compared against.
Anyone making the decision today between a GLP-1 and waiting is comparing the current tirzepatide reality, not a speculative future drug.
What brenipatide is and where it is headed
Brenipatide is structurally a cousin of tirzepatide. Both are peptides that activate the same two receptors. The interesting engineering choice was on the peptide backbone. Lilly swapped a tryptophan residue for an α-methyl-tyrosine, which makes the molecule resistant to the proteases that normally chew up GLP-1 analogs in circulation. Net effect: brenipatide hangs around in the blood for weeks rather than days, which is why it can be dosed once a month subcutaneously instead of weekly.
That dosing schedule is the central feature, and it is also the reason Lilly is leading with alcohol use disorder rather than obesity. For weight loss, weekly injections are tolerable for motivated patients. For someone trying to stop drinking, the friction of a weekly self-injection is exactly the kind of decision a relapse looks for. Monthly dosing solves that. The clinical analog already exists. Naltrexone for AUD comes as both a daily pill and a monthly intramuscular shot (Vivitrol), and the monthly form consistently outperforms the daily one for the same reason: people who have stopped drinking actually stay on it.
Lilly is also testing brenipatide in major depressive disorder and bipolar disorder, which is a meaningful pivot of the GLP-1 class into psychiatric indications. The broader pattern of GLP-1 drugs reducing addictive and compulsive behavior has shown up across multiple datasets, including a 606,000-veteran cohort published in BMJ earlier this year showing meaningful reductions in alcohol, nicotine, and opioid use disorder rates in GLP-1 users. Brenipatide is the first molecule in the class engineered around that signal rather than around hunger.
The catch, and it is a real one, is that none of the brenipatide trial results are out yet. We do not have published weight-loss numbers, we do not have head-to-head efficacy data against tirzepatide, and we do not have a real-world side-effect profile. Everything available right now is mechanism, dosing schedule, and pipeline status.
For the full case on the addiction angle, I wrote up the brenipatide AUD story separately. This post is the head-to-head comparison.
Brenipatide side effects: what is actually known
The honest answer is that there is no published brenipatide side-effect profile yet. The Phase 3 alcohol-use-disorder trials, RENEW-ALC-1 and RENEW-ALC-2, are still enrolling, and the first real tolerability data is not due until 2027. So anyone selling you a brenipatide side-effect list today is either describing the GLP-1 class in general or guessing.
The only honest way to talk about it right now is from the receptors it hits. Brenipatide works on the same GLP-1 and GIP receptors as tirzepatide, so I would expect the same gastrointestinal package the whole class produces: nausea, vomiting, constipation, less appetite, worst while the dose is climbing. In the tirzepatide trials about 6 to 7 percent of people quit over side effects. That is the bar this one will get measured against.
The monthly dose is the part nobody can call yet. One shot a month means a higher peak right after you inject and a long fade before the next one, which is a different curve than a weekly drug. Maybe that makes the first few days after each shot rougher. Maybe it stretches the adjustment out and makes it easier. We just do not know until the data lands.
The part I would actually keep an eye on has nothing to do with nausea. Because brenipatide is being tested in psychiatric patients, the trials are watching mood and behavior much more closely than an obesity study ever would. That is the piece of the brenipatide story that will not look like any GLP-1 before it, and it is the real reason I care about the 2027 readouts.
Brenipatide and weight loss: why there are no numbers yet
The question I get most is whether brenipatide is a weight-loss drug. It is not, at least not the way Zepbound is. Lilly built it for neuroscience, and the biology is tuned toward addiction and psychiatric endpoints, not maximum appetite suppression. The obesity program is still stuck in Phase 1, years behind the alcohol trials.
That is why there are no brenipatide weight-loss numbers to quote. No trial has reported how much weight people lose on it, because those trials have not read out. Any specific percentage you see next to brenipatide right now is borrowed from another drug or made up.
Will it drop some weight anyway? Probably a little, because every GLP-1 and GIP agonist takes the edge off appetite. But weight loss as a side effect is a different thing from the 22 percent tirzepatide delivers on purpose, and Lilly has given no sign it wants to run brenipatide as an obesity drug while the addiction work is the priority.
If your real question is weight loss, I would not wait on brenipatide. The useful data is elsewhere. Tirzepatide has the Phase 3 record and is in pharmacies today. Retatrutide, the triple agonist behind the biggest weight-loss numbers anyone has posted so far, is the one I would actually read up on. Brenipatide is the one to watch for sobriety and mental health, not for the scale.
The differences that actually matter
If you are trying to decide between the two drugs for any practical purpose, this is the comparison that matters:
| Tirzepatide | Brenipatide | |
|---|---|---|
| Dosing | Weekly subcutaneous shot. | Monthly subcutaneous shot. |
| Primary indication | FDA-approved for type 2 diabetes, obesity, and obstructive sleep apnea. | Phase 3 for alcohol use disorder. Depression and bipolar also in development. Obesity only in Phase 1. |
| Efficacy data | Multi-year, large Phase 3 trials. SURMOUNT-1 showed about 22.5% weight loss at 72 weeks. | No published trial results yet. Extrapolating from the GLP-1 class. |
| Availability | In pharmacies now. | Trial-only. Gray-market knockoffs are unlikely for years because the monthly backbone is hard to copy. |
| Cost | About $299/month through LillyDirect for self-pay. Often less with insurance. | Not on the market. Pricing unknowable today. |
| Timeline | Available now. | Plausibly 2029 or 2030 if Phase 3 readouts in 2027 are positive. |
| Side effects | Well characterized. Mostly gastrointestinal. About 6–7% discontinue for side effects. | Profile not yet public. Monthly dosing might soften peak GI effects or extend the adjustment window. |
The structural takeaway from that comparison is simple. Tirzepatide is a finished product for the problem it was designed to solve. Brenipatide is a new product for problems that mostly have not had a great drug before.
Should you wait for brenipatide?
If you are looking at this as a weight loss decision, no. Brenipatide is unlikely to be approved for obesity in any meaningful timeframe. Even if Lilly chases the obesity indication as a second label, the AUD trials are the priority and the Phase 1 obesity program is years behind. By the time brenipatide is on shelves for weight, tirzepatide will have eight years of real-world data, deeper insurance coverage, and almost certainly other dual or triple agonists in the same competitive space (retatrutide is the obvious next one to land).
If you are looking at this for alcohol use disorder, or for a craving-driven problem like nicotine relapse or compulsive behavior, the calculus is different but the answer is still mostly no, because brenipatide is not available outside a trial. The practical version of the right question is whether you should consider an off-label semaglutide or tirzepatide trial for AUD now, given the existing data, rather than waiting for the on-label option in 2029. That is a real conversation to have with a doctor who has read the JAMA Psychiatry semaglutide AUD trial. It is not a do-it-yourself problem.
If you are following this as a longevity or “what is coming next” question, brenipatide is the right thing to watch. The combination of monthly dosing, a new indication category (neuroscience instead of cardiometabolic), and the broader GLP-1-and-addiction signal is the most interesting pipeline development in this class right now. The 2027 readouts are the milestone to mark.
For most people reading this, the practical question is not “should I wait for brenipatide?” but “should I be on a GLP-1 at all, and if so, which approved one?” That is the question tirzepatide already has an answer to.
I keep a running tracker of every GLP-1 and incretin drug, approved and still in the pipeline, with what each one targets, how far along it is, and what's coming next.
See the full GLP-1 Pipeline Tracker →About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.