
The most effective weight-loss drug yet seen in large trials still isn’t approved. It already has a street name, a grey market with customer service, and a fan base that includes people who were never obese. I own the drugmaker’s stock, and I still wouldn’t touch the vials.
I give myself a Zepbound shot every week. It’s an approved drug, my doctor prescribes it, and it has quietly rebuilt my metabolic health over the past couple of years. So it’s a strange feeling to watch a different injection, one nobody can legally buy, become the drug everyone actually talks about.
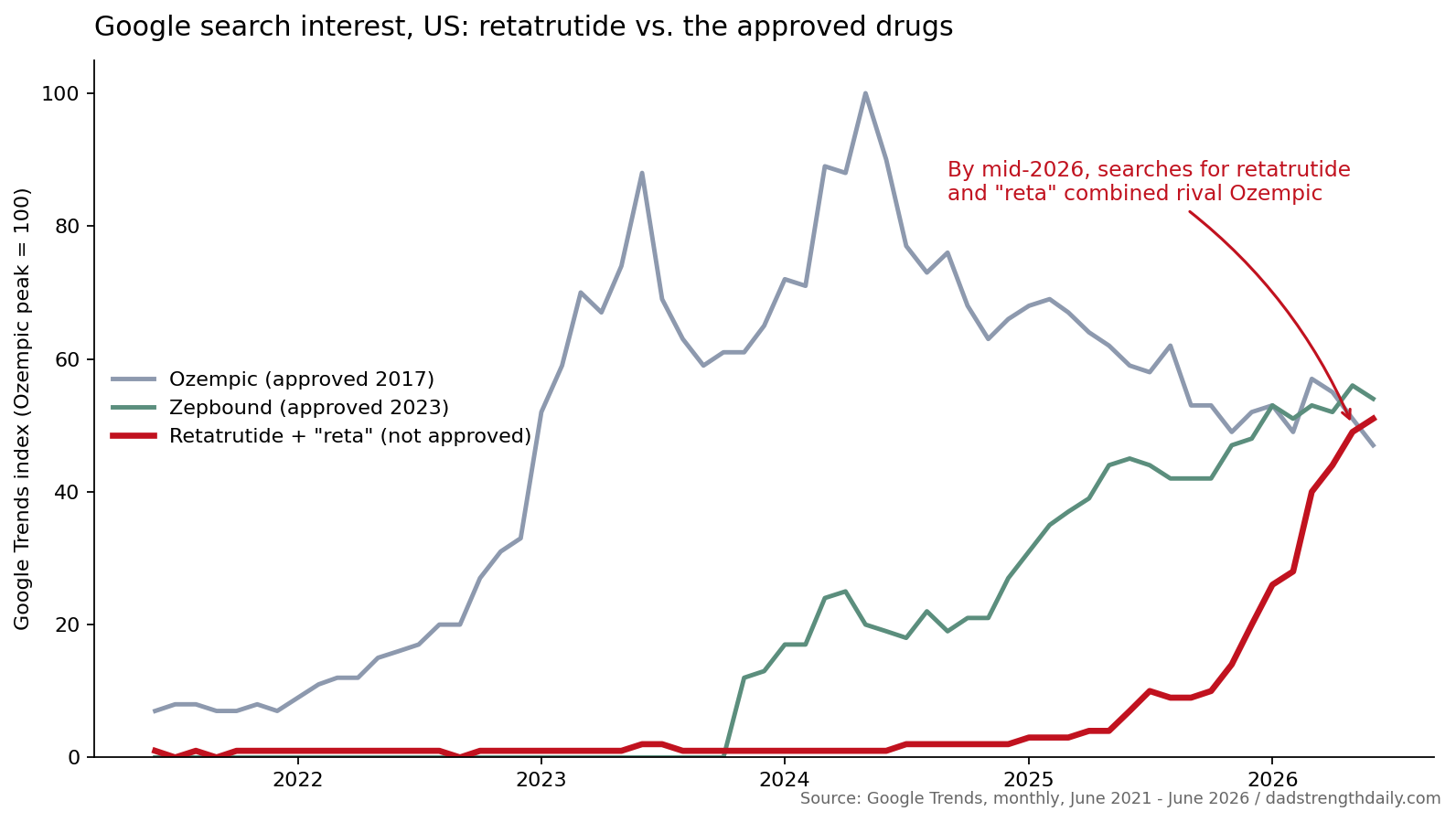
The drug is retatrutide. Eli Lilly is still running its Phase 3 trials. The FDA hasn’t reviewed it. Your pharmacy has never stocked it. And in early June 2026, for the first time, Americans googled it about as often as they googled Ozempic.
Think about how backwards that is. Ozempic is a household name, the most famous medication of the decade. Retatrutide is an experimental compound that Lilly’s own website warns you not to buy. The search interest crossed anyway. It has a street name (“GLP-3”), a thriving grey market, forums with tens of thousands of members comparing doses, and a customer base that runs from people with severe obesity to bodybuilders cutting for summer to startup founders who think it sharpens their focus. The Atlantic’s Sarah Zhang opened her December piece on the underground market with a woman whose hairdresser was already on it.
I think retatrutide is the inflection point for this whole class of drugs. Not just because of what it does in trials, although that part is genuinely historic, but because of what’s happening around it. A drug this strong, with this much demand before approval, is already reshaping the market around it, from the people using it to the company that makes it, and it isn’t even approved yet. Here’s the part that complicates it for me: I inject a GLP-1 every week, I own Lilly stock, and I still would not put grey-market retatrutide in my own body. The rest of this is why.
Full disclosure, because it colors all of this: I’m on Zepbound, Lilly’s tirzepatide, so I have skin in this as a patient, and I bought Eli Lilly stock about a year ago, partly because I believed exactly the story this post tells. It’s up roughly 40 percent since, against about 20 for the S&P 500.
The trial result that drew comparisons to surgery
In TRIUMPH-1, Lilly’s pivotal obesity trial with 2,339 participants, people on the highest dose lost an average of 28.3 percent of their body weight over 80 weeks. That’s about 70 pounds. The heaviest participants, followed out to two years, lost 30.3 percent, around 85 pounds. The comparison that landed for me came from the New York Times: that’s in the range of gastric bypass surgery, which delivers 30 to 35 percent at two years and has long been the only reliable treatment for severe obesity. The trials aren’t head-to-head and long-term durability is still an open question, but a drug reaching surgical-range weight loss is genuinely new.
For comparison, Zepbound and Wegovy top out around 20 percent. The leading oral GLP-1 pills land somewhere between 12 and 14. When Lilly presented retatrutide’s early Phase 2 numbers at a medical conference in 2023, a scientist in the room told The Atlantic the usually staid audience broke into spontaneous applause. Endocrinologists do not normally applaud slide decks.
There’s a detail in the trial reports I keep retelling people. Some participants quit because they felt they were losing too much weight. Lilly’s own release on the knee-osteoarthritis trial says people dropped out “for perceived excessive weight loss.” Think about how odd that sentence is in obesity medicine. For decades the field’s problem was that safe, scalable drug treatment rarely produced anything close to this. Now a company is fielding complaints that its drug works too hard.
And the weight is only part of the package. In the diabetes trial published in The Lancet in June 2026, retatrutide as a first drug drove blood sugar to near-normal levels in early type 2 diabetes while taking off 15.3 percent of body weight. The knee trial cut osteoarthritis pain scores by roughly three quarters. A liver substudy, an earlier Phase 2 secondary finding, showed the drug cleared fatty liver in most people on the higher doses, and there are programs running in sleep apnea, chronic kidney disease, and low back pain. Lilly talks about retatrutide less like one more shot and more like the anchor for a family of obesity-complication treatments. But remember what these are: early, mostly condition-specific results in people who already have obesity. One drug doesn’t fix everything.
The mechanism is simple enough to hold in your head. Wegovy mimics one gut hormone, GLP-1. Zepbound mimics two, adding GIP. Retatrutide adds a third, glucagon, which seems to push energy expenditure up by revving the liver while the other two suppress appetite. That third lever is also where some of the heart-rate and tolerability questions come from, which I’ll come back to. The grey market’s “GLP-3” nickname is chemically wrong and culturally perfect.
Get the next one in your inbox
I write about longevity, training, and preventive health weekly — without the guru worship. Free, no spam, unsubscribe whenever.
The grey market got there first, and it’s not hiding
What’s strange is the timing. By the time those Phase 3 results landed in May, plenty of Americans had already been injecting retatrutide for two years. Not study volunteers. Customers.
Nobody can count them precisely, which is the nature of an underground market. But the signals are everywhere. Reuters profiled the do-it-yourself GLP-1 scene last summer and found one Telegram community alone with more than 21,000 members; the lab it tracked tested about 3,050 grey-market obesity-drug samples in 2024, up from roughly 650 the year before. US customs data show imports of hormone and peptide compounds from China doubled in a year, to $328 million in the first three quarters of 2025. The FDA has sent warning letters naming retatrutide to online sellers, one as recently as March.
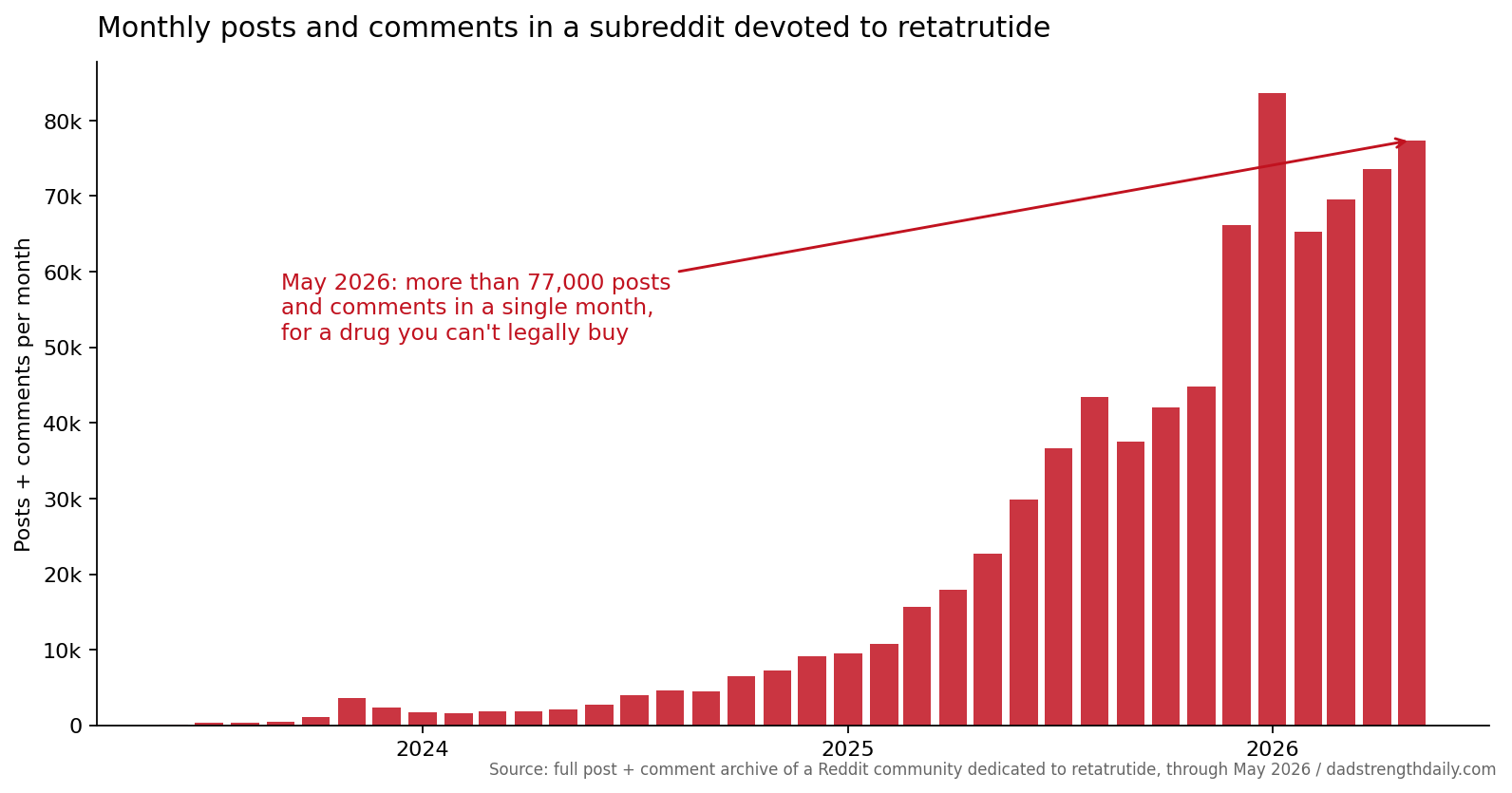
The clearest signal is sheer volume. There is an entire subreddit devoted to retatrutide, and I pulled its full archive. In mid-2023 it ran a few hundred posts a month. By May 2026 it was logging more than 77,000 posts and comments a month, for a drug nobody can legally buy. That isn’t a fringe forum. That’s a town.
What changed wasn’t just scale. It was texture. The early adopters, around 2024, were the people you’d expect: bodybuilders and biohackers wiring crypto to Chinese sales reps on Telegram. I wrote about that scene when the first Phase 3 topline dropped. Since then the market has grown a friendly storefront layer. Slick American reseller sites take PayPal and credit cards. Influencers post affiliate discount codes for “reta.” One vendor shipped Zhang’s Atlantic order with a Shop-app tracking link, an experience she described as feeling like ordering socks. The vials still say “research use only,” but that’s a legal fiction nobody bothers to maintain in conversation. When a popular Substack guide to cheap weight-loss drugs named retatrutide its top pick, a vendor responded with a 15-percent-off discount code for readers.
The creator economy tells the same story. Search the drug’s name on YouTube and you’ll find beginner’s guides, titration tips, and “avoid these retatrutide mistakes” videos with half a million views, some sponsored by electrolyte brands, alongside Good Morning America and CBS segments. Peter Attia gets asked about it enough that he answered it on a recent podcast. An experimental compound with fan content and morning-show coverage isn’t a black market. It’s a product launch the manufacturer never scheduled.
I spent an evening in June 2026 reading the largest grey-market GLP-1 forum, the kind of place this trade actually lives. I expected something seedier. It has nearly 60,000 registered members. Its retatrutide section holds 570 threads and almost 13,000 posts, more than its tirzepatide section, which covers a drug you can get prescribed tomorrow. The top thread when I visited was “What dose of reta are you at?”, last reply 31 minutes earlier. A dozen Chinese suppliers run official vendor accounts there, posting US-warehouse promotions with emoji the way a mattress store announces a Presidents Day sale. There’s a crypto-payments board, a group-testing schedule, and a lab-results section where one recent thread reports a vial that contained no drug at all.
A companion site for newcomers describes itself, without irony, as “the Consumer Reports of gray market tirzepatide,” with beginner guides to reconstitution, vendor selection, and a “Crypto 101” explainer. Its manifesto line is the purest statement of the normalization I’ve seen anywhere: “Gray isn’t just a market; it’s a mindset. It’s about stepping up when the healthcare system stepped out.” However you judge the choice, notice the register. That’s not the voice of people who think they’re doing something shady. It’s the voice of a consumer movement.
The market also polices itself, after a fashion. An entire cottage industry of labs has grown up to check what the vendors ship, and the most trusted name in it is Janoshik, a Slovak lab whose single most popular product is built for exactly this moment. You send in an unlabeled vial, you don’t even have to say what you think is in it, and for $360, payable in crypto, the lab identifies whether it holds semaglutide, tirzepatide, or retatrutide and measures how pure it is. The founder says peptides went from a sideline to roughly three-quarters of his business in two years, once GLP-1 demand exploded. Buyers send samples, vendors post the certificates, group buys get tested batch by batch. Blind testing like that, he told one interviewer, is “what’s actually keeping everyone in check, including us.” Rory Hester, who covers the scene and recently co-founded a peptide company himself, told Zhang the line I can’t stop thinking about: “The future of the market is normies.” Your grandmother won’t use Telegram. She will absolutely use a checkout page with PayPal.
The testing culture sounds reassuring until you look at what the labs find. A 2026 preprint went big, analyzing more than 6,400 grey-market samples across fourteen compounds, retatrutide among them. Depending on how strict the standard was, between 42 and 71 percent failed basic quality checks, and 15 percent of the samples screened for endotoxin carried measurable bacterial contamination, the kind that causes fevers, chills, and in the worst case septic shock. The consumer-facing labs that publish their own running numbers come in lower, in the 10-to-20-percent range, but they only test what customers choose to send them. Different pools, different yardsticks, so don’t read them as one figure, but the direction holds. Mostly, the powder is what the label claims. “Mostly” carries a lot of weight in a product you inject weekly.
The supply chain has the failure modes you’d expect. Two of the most popular Chinese suppliers vanished in September, mid-order, amid rumors of arrests. In November, warnings spread that another vendor’s batch had put two people in the hospital, followed by impersonation scams and counter-rumors that the whole episode was a hoax. There’s no recall system in an underground market. There’s just the group chat, deciding together what to believe.
And the people injecting are now their own clinicians. The most sobering detail in Zhang’s reporting wasn’t a contamination number. It was a 62-year-old who has been on grey-market retatrutide for a year and a half, longer than any participant in the completed trials, dosing herself off the published protocol, and who has never told her doctor any of it.
The customers were never just obese people
If the grey market only served people with severe obesity who couldn’t wait for the FDA, this would be a simpler story about desperation and a slow approval pipeline. It isn’t.
A KFF survey found that by late 2025, one in eight American adults said they were currently taking a GLP-1 drug. That’s the approved ones. Retatrutide is the aspirational tier above them, and its early adopters increasingly look nothing like the trial population. Nobody has real demographic data on grey-market buyers, so what follows is reporting and observation, not a census. The New York Times ran a piece in January on “Chinese peptides” as the new status drug of the tech world. Peptide raves in San Francisco with mix-your-own workshops. A supplier who says adoption inside a company “always starts with the CEOs.” And retatrutide specifically being taken not for weight but for “everything from appetite suppression to increased focus.” One startup chief executive in that story added retatrutide to her routine to help her quit vaping. Her hair started falling out within a month because she was eating so little, and her overnight heart rate jumped 10 beats per minute. She plans to keep going.
A 29-year-old founder in the same piece switched herself from prescription Zepbound to grey-market retatrutide after a conference session suggested it, citing the pressure of looking good in launch videos. “Founders aren’t overweight,” she observed. She’s not wrong about the observation. That’s what makes it chilling.
The first GLP-1 wave was sold, and mostly used, as medicine for a disease. The retatrutide wave is being adopted, pre-approval, by people chasing lean. Bodybuilders running it on a cut. Normal-weight men and women who want visible abs and have read this is the strongest tool ever made. People treating appetite itself as a bug to be patched. I’ve written about bigorexia and the comparison culture that runs on photos, and about how biohacking turned into shopping. Retatrutide is where all of that meets real pharmaceutical power. The drug can deliver bariatric-surgery weight loss, over two years and at the highest doses. Aim that at someone who starts with a BMI of 24, and nobody can tell you what happens, because no trial has ever asked.
Lifters should hear one number in particular. In the trial data so far, a meaningful share of the weight lost on these drugs isn’t fat. DEXA substudies across the class suggest somewhere between a quarter and a third of the loss can be lean mass, and the early retatrutide figure sits at the high end of that range, with the usual caveats about what DEXA actually measures. In practice that looks like your bench press dropping while the scale flatters you. The grey-market crowd talks about “reta” as a shortcut to stage-lean. Elizabeth, the 62-year-old in the Atlantic piece, put the other side plainly after losing 100 pounds: “I’m as weak as a kitten.” Protein and a barbell are not optional accessories to these drugs. They’re the difference between losing weight and losing yourself.
Even inside the trials, with medical supervision, the dosing conversation is getting delicate. The Times reported in February that doctors are already wrestling with patients who hit every metabolic target and want to keep going. One Michigan obesity physician put it bluntly: society has trained us toward beauty standards that aren’t health standards, and an injection that makes starvation easy demands more caution, not less. On the grey market, where the prescriber, pharmacist, and patient are the same person, that caution rounds to zero.
There are open safety questions, and they’re not small. The glucagon part of the drug can nudge heart rate up. In the Lancet diabetes trial, seven of 403 people on the drug had arrhythmias and three had major cardiovascular events, against none on placebo. The investigators are explicit that the numbers are too small to conclude anything, and the lipid, blood pressure, and weight improvements all point the right way. But the dedicated cardiovascular outcomes trial doesn’t read out until around 2029. There’s also dysesthesia, a burning, prickling skin sensation that hit roughly one in eight high-dose patients in the obesity trial and up to one in five in the knee trial, something earlier GLP-1s mostly don’t cause. And 11.3 percent of high-dose participants quit the pivotal trial over side effects, about double the placebo rate. None of that is disqualifying for a supervised drug in heavy patients. All of it matters more when a lean 30-year-old is eyeballing doses from an unlabeled vial.
Wall Street already wrote the ending
My disclosure matters most here: I own Lilly shares, so discount accordingly.
Lilly became the first healthcare company worth a trillion dollars in late 2025, built substantially on tirzepatide, and in the first quarter of 2026 alone it booked $19.8 billion in revenue. Retatrutide is positioned as the next layer: the maximum-strength option for people who need surgical-scale weight loss, stacked on the shots and pills the company already sells, with the osteoarthritis, sleep apnea, liver, and kidney programs widening the label over time. Citi has called it a potential category-defining franchise, and after the ADA data its analysts argued even the lowest dose belongs in first-line use. Bloomberg reports estimates for retatrutide alone building past $10.6 billion a year by 2036, which would make it one of the biggest drug launches ever.
There’s a quieter signal of how seriously Lilly takes the long game: it sued the FDA in 2024 over whether retatrutide counts as a “biologic,” a classification worth billions because it would extend Lilly’s pricing power and block competitors for years. That fight is still unresolved, and the whole argument turns on a single amino acid. Companies don’t litigate that over a product they expect to be modest.
Here’s the wrinkle my own brokerage account taught me. When the bariatric-surgery-grade results landed in May, the stock moved a few percent and settled. The result everyone called historic was already in the price. Lilly trades at more than double the earnings multiple of Novo Nordisk precisely because investors assume retatrutide and the oral pipeline deliver. So the things to watch aren’t more weight-loss headlines, and I’ll keep logging them in the GLP-1 pipeline tracker. They’re the readouts that decide insurance coverage and label breadth, starting with the trial in people with obesity and established cardiovascular disease, which finished in spring 2026 with results expected later this year. Then the FDA filing, then a likely launch around 2027. Attia told his audience he expects approval barring a disaster, and he’s hardly alone, though the cardiovascular and longer-term safety data still have to hold up, which matters more for a drug that adds glucagon.
The headwinds are real too, and they’re about money rather than molecules. Goldman Sachs recently cut its obesity-market forecast to $95 billion by 2030, citing pricing pressure and how many people quit the drugs; Morgan Stanley sees the broader GLP-1 market reaching $190 billion by 2035. Reuters reported in June 2026 that some large employers are weighing dropping GLP-1 coverage for weight loss in 2027 because the bills are stressing benefit budgets. A maximum-strength premium drug arriving into that fight will launch with insurance restrictions, not open arms. And hanging over all of it, the question nobody models well: how many grey-market customers convert to a branded product that will plausibly cost ten times what a Chinese supplier charges? I have no idea how to model that, and I doubt the analysts do either. What the underground market has done, whether Lilly likes it or not, is spend two years proving how many people want this drug badly enough to import it from China. Marco, one of Zhang’s sources, has a year’s supply in his freezer and plans to keep buying for friends after approval. The street price is now a competitor.
Why my own shot isn’t changing
After a year of watching this drug mint converts on Reddit and fatten my brokerage account, you might expect me to be first in line. I’m not. My reasons are boring, which is sort of the point.
Tirzepatide is working for me. The weight came off and stayed off, my blood work looks better than it has in a decade, and the weekly shot is now as routine as taking out the recycling. Switching to something stronger would solve a problem I don’t have. The trial data on retatrutide’s extra tolerability cost, the doubled dropout rate, the skin sensations, the unanswered heart-rhythm question, is exactly the kind of trade I don’t need for a goal I already hit. More isn’t a treatment plan.
The grey-market version was never on the table, even though I understand the pull better than most. I inject a peptide weekly. I know the copay pain that drives people to Telegram. But there are two separate gambles in those vials, and people keep talking about them as one. The molecule itself is still being characterized, even in Lilly’s hands. And the powder in an unlabeled vial may not be that molecule at all. The product fails independent testing anywhere from 10 percent of the time at the clean end to well over 40 percent in the largest sample, there’s no completed long-term safety picture even for the pharmaceutical-grade version, and the entire risk-management apparatus is a certificate of analysis posted by the people selling it. My doctor knows every milligram I take. That’s not timidity. At my age, that’s the whole strategy.
Attia is more aggressive about prevention than almost anyone in this space, and even he tells patients the same thing. Asked whether they should be getting grey-market retatrutide, his answer is blunt: no, you should not. Use tirzepatide until the drug is approved.
If retatrutide is approved on schedule, somewhere around 2027 a doctor will be able to prescribe the real thing, manufactured to pharmaceutical standards, with a label that reflects whatever the cardiovascular data show and a titration plan supervised by someone who can order an ECG. For people with severe obesity, the ones the drug was actually built for, that’s going to be a very big deal if the safety and durability data hold up: surgery-level weight loss from a weekly shot, under real medical supervision. For everyone else, the lean-chasers and the founders judging themselves against launch videos, the honest answer is that nobody has studied you, and the strongest tool is rarely the right one for the smallest job.
The inflection already happened. America didn’t wait for the FDA to take a drug like this. I’m going to. I’ll stay on the sidelines, with the shot my doctor actually prescribes.
About Gunnar
Gunnar is 53. He lost about 170 pounds, trains in a garage gym, and writes DadStrengthDaily from personal experience, citing primary sources where he can. He also moderates r/ProactiveHealth. He is not a doctor, and nothing here is medical advice. Talk to your own doctor before acting on anything, especially GLP-1s, TRT, blood pressure, sleep apnea, and cancer screening.